










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



An early clinical trial in individuals with the deadly brain cancer, glioblastoma, showed an experimental spherical nucleic acid (SNA) drug developed by Northwestern University scientists was able to penetrate the blood-brain barrier and trigger the death of tumor cells.
This is the first time a nanotherapeutic has been shown to cross the blood-brain barrier when given through intravenous infusion and alter the genetic machinery of a tumor to cause cell death. The drug crossed the blood-brain barrier, dialed down the level of a cancer-causing gene and promoted tumor cell death.
The Northwestern Medicine study will be published March 10 in Science Translational Medicine. The results build upon previously published pre-clinical research by the Northwestern team.
“We showed the drug, NU-0129, even at very small doses, causes tumor cells to undergo what’s called apoptosis or programmed cell death,” said lead investigator Dr. Priya Kumthekar, an associate professor of neurology at Northwestern University Feinberg School of Medicine and a Northwestern Medicine physician.
“It’s a remarkable finding in humans that confirms what we had previously seen in our animal studies.”
In phase 0, investigators use a small dose of medication to make sure it isn’t harmful to humans before they start using it in higher doses in larger clinical trials.
Study participants received the drug intravenously prior to surgery. Following tumor removal, Kumthekar and her team studied the tumors to determine how well the drug crossed the blood-brain barrier and its effect on the tumor cells.
Glioblastoma affects approximately 13,000 to 15,000 patients each year in the United States and is uniformly fatal. There have been no new drugs approved for glioblastoma in the past decade. Scientists said it’s been hard to develop a drug that can breech the protective blood-brain barrier and reach the highly aggressive brain tumor.
SNAs look like a Koosh ball
“This unique 3D design has the ability to infiltrate tumor cells to correct the genes inside and make them susceptible for therapy-induced killing,” said senior author Alexander Stegh, an associate professor of neurology at Northwestern.
NU-0129 is the first SNA drug developed for systemic use. SNAs are structures consisting of of DNA or RNA arranged around a nanoparticle, which looks like a Koosh ball, Stegh said.
Stegh developed the drug with Chad A. Mirkin, the discoverer and inventor of the SNA platform and the George B. Rathmann Professor of Chemistry at the Weinberg College of Arts and Sciences and director of Northwestern’s International Institute for Nanotechnology.
The glioblastoma drug represents a revolutionary new class of drugs.
The novel SNA platform on which it is based can be applied to other types of neurological diseases, such as Alzheimer’s, Huntington’s and Parkinson’s, by similarly turning down the genes that lead to those diseases.
Highly unusual drug route
It’s highly unusual for a drug to be developed in preclinical research at a university, shepherded through U.S. Food & Drug Administration approval as an investigational new drug and studied in a clinical trial – all within the same university and without funding from a pharmaceutical company. In most cases, a drug is developed and licensed to a pharmaceutical company.
“We want to move the technology forward as quickly as possible because there are patients with a disease with no current cure,” Kumthekar said.
Dr. Leon Platanias, director of the Lurie Cancer Center, said, “These exciting findings for the first time support the potential of spherical nucleic acids for drug delivery to brain tumors. They may prove to have important long-term translational implications for the treatment of these tumors.”
Non-viral Vectors for Gene Therapy
Non-viral vectors are emerging as attractive platforms for gene therapy approaches for GBM. Recent studies discussed below, have demonstrated the potential of these delivery technologies.
Non-polymeric Delivery System
Liposomes
Liposomes are artificial, lipid-based microvesicles that are considered as a possible valuable system to achieve therapeutic efficacy in glioma. On this backdrop, a liposomal vector was devised in early 2000s to carry a plasmid coding for HSV-TK which was given to patients with recurrent GBM in a Phase I/II trial via intratumoral infusion, followed by administration of the prodrug ganciclovir (Reszka et al., 2005).
This therapy was well-tolerated without major side effects. Also, they observed >50% reduction of tumor volume in patients. Although this was a small Phase I trial and thus, it was not powered to determine therapeutic efficacy. Moreover, Kato et al. demonstrated that siRNA-based downregulation of MGMT could enhance the chemosensitivity of malignant gliomas against TMZ using novel liposome, LipoTrust EX Oligo.
Such liposome transduced glioma cells are found to be sensitized to TMZ both in vivo and in vitro models (Kato et al., 2010). A dual targeting with T7 and A7R peptides was developed to target vascular endothelial growth factor receptors 2 (VEGFR2) (Zhang et al., 2017). PEG-conjugated liposomes modified with the Transferrin receptor (TfR) monoclonal antibody (OX26) and chlorotoxin (CTX) significantly promoted cell transfection, increased the transport of plasmid DNA bearing hTERTC27 gene across the BBB and efficiently targeted brain glioma cells both in vitro and in vivo.
This dual targeting therapeutic strategy of OX26/CTX-pL/pC27 against glioma exhibits significant therapeutic efficacy leading to diminished tumor volume and extended survival of glioma bearing rats (Yue et al., 2014). Other liposomal formulations with modified surface and core include magnetite-core cationic liposomes that can be used to activate a heat-shock sensitive promoter in the DNA carried by the liposome, thus regulating expression of the therapeutic gene such as TNFα in glioma cells (Ito et al., 2000).
Nanoparticles
NU-0129 is a spherical nucleic acid gold nanoparticle containing siRNAs targeting Bcl-2-like protein 12 (Bcl2L12) is now in early phase I clinical trials (NCT03020017) for patients with recurrent glioblastoma. It can cross BBB in xenograft GBM mice after systemic administration which results in increased apoptosis of glioma cells and reduced tumor progression (Jensen et al., 2013).
RNA nanoparticles are also used to deliver anti-miR-21 in xenograft GBM mice, resulting in tumor regression and increased survival (Lee et al., 2017). Intravenously-administered chlorotoxin (CTX) coupled stable nucleic acid lipid particle (SNALP) formulated anti-miR21 oligo preferentially accumulates within the brain tumor and efficiently silence miR21 expression.
This results in increased mRNA and protein levels of RhoB, leading to reduced tumor load and proliferation without inducing any systemic immunogenicity (Costa et al., 2015). Moreover, combined treatment of both nanoparticles formulated anti-miR21 oligo and tyrosine kinase inhibitor Sunitinib exerts enhanced apoptosis and improved survival in mice (Costa et al., 2015).
Development of a library with PBAE based nanoparticles carrying herpes simplex virus type I thymidine kinase (HSV-TK) DNA, resulted in apoptosis of transfected glioma cells. This led to increased median survival of glioma bearing animals when delivered intracranially (Choi et al., 2020). Furthermore, when HSV-TK DNA loaded nanoparticles are delivered in combination with the prodrug ganciclovir (GCV) to glioma cells in vivo, they elicited induction of apoptosis and reduction of tumor load in glioma bearing rats (Mangraviti et al., 2015).
Another important type of anti-GBM treatment in gene therapy uses different types of RNA such as dsRNA, siRNA or miR101 associated to nanoparticulate systems resulting in enhanced apoptosis of GBM cells. Also inhibition of growth and migration of these cells can be induced through targeting miR34 or proteins like SOX9 and Ras with the same nanoparticulate systems (Shu et al., 2014; Kim et al., 2015b; Alphandery, 2020).
We have recently demonstrated that local treatment of glioma with sHDL (synthetic High-density lipoprotein) mimicking nanodiscs containing ApoAI mimetic peptide, phospholipids, immunogenic cell death inducing chemotherapeutics (ICD) docetaxel and adjuvant CpG oligodeoxynucleotide, effectively elicit anti-glioma T-cell activity and induce immunological memory response against tumor relapse (Kadiyala et al., 2019).
We also engineered an albumin based NPs equipped with cell-penetrating iRGD peptide, containing siRNA against Signal Transducer and Activation of Transcription 3 factor (STAT3i) and demonstrated that when administered in combination with ionizing radiation, these NPs activate anti-GBM immunologic memory which results in tumor regression and long term survival of GBM bearing mice (Gregory et al., 2020).
Other peptide modifications on nano-platforms have been explored to minimize off-target accumulation and facilitate active tumor targeting or mediate BBB transport. For example, IL-13Rα2 is overexpressed on glioma cells, therefore it is an attractive target for peptide-modified nanotherapies (Madhankumar et al., 2006). A study revealed that IL-13-conjugated nanoplatform enhanced therapeutic efficacy in a subcutaneous mouse model of glioma (Madhankumar et al., 2006).
Moreover, transferrin receptor (TfR) has been extensively researched as a target for gliomas, because TfR is over-expressed on glioma cells (Kang et al., 2015). Despite exploiting the use of TfR as a target for decades, translation of systems leveraging these finding have been limited (Johnsen et al., 2019). On this backdrop, a seven amino acid peptide (sequence: HAIYPRH, T7), which has a greater affinity for TfR has been used for glioma targeting to deliver siRNA (Wei et al., 2016), coupled with other targeting ligands to demonstrate increased transport across the BBB and greater tumor penetration (Zong et al., 2014).
Oncolytic Viruses
Several oncolytic viruses have been evaluated in preclinical studies or clinical trials for the treatment of GBM. Specificity must be seriously evaluated, taking into consideration the infection capacity of the vector. Oncolytic viruses (OVs) are designed to recognize tumor receptors or to replicate under oncogene promoters in order to improve their tropism and avoid non-neoplastic cells.
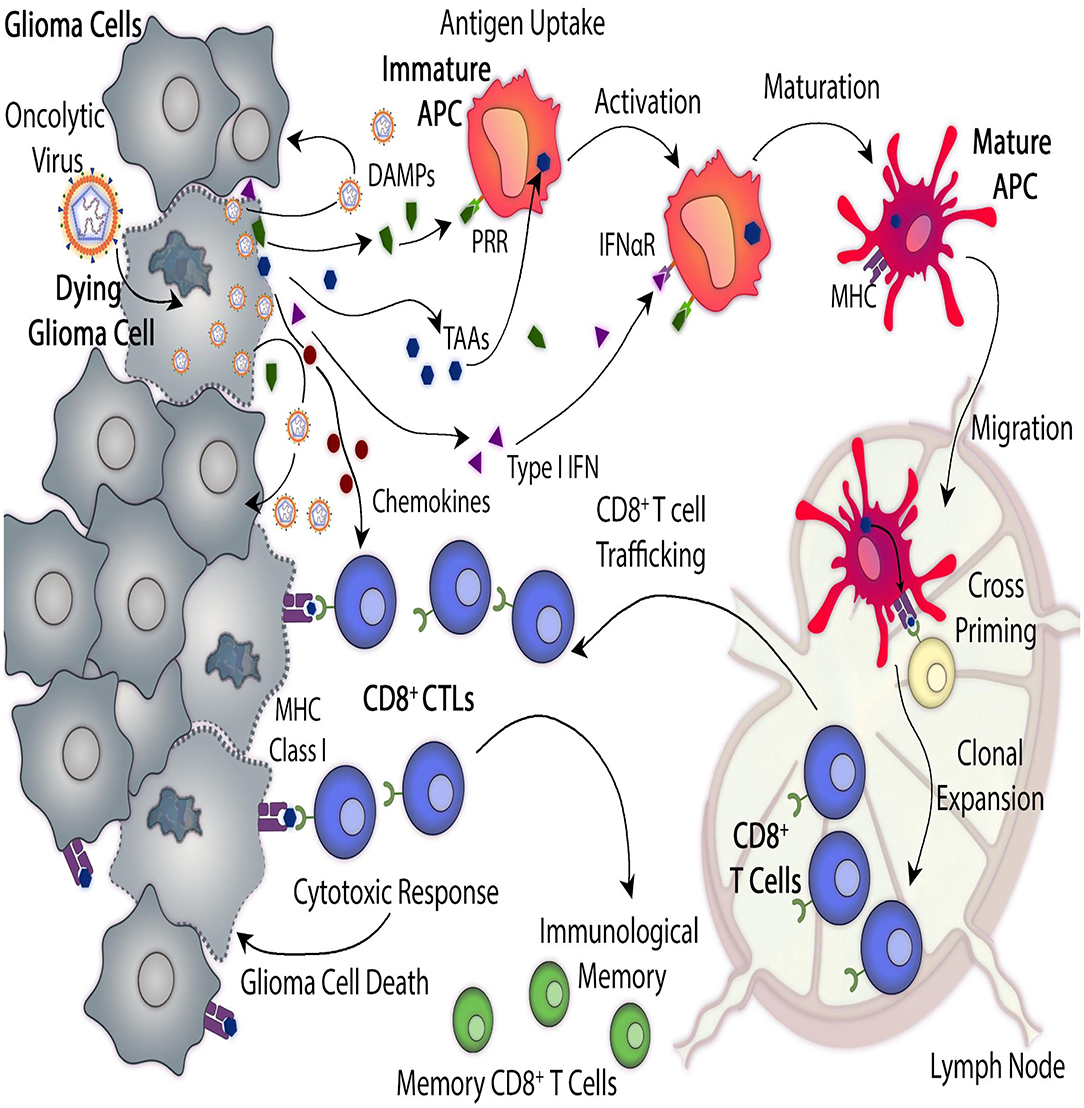
It was observed that the immunosuppression present in the tumor microenvironment promotes the OV infection capacity and improves the oncolysis (Tobias et al., 2013; Davola and Mossman, 2019). Once infected, the dying tumor cells start the presentation of tumor epitopes, triggering a viral-specific and tumor-specific T cell-mediated immune response, critical for the efficiency of the oncolytic virotherapy (Li et al., 2017).
When tumor cells are lysed, tumor-associated antigens (TAA) are released into the tumor microenvironment and recognized by the immune system, which stimulates the recruitment of activated immune cells which overcome the tumor-mediated immunosuppression and activate a systemic response (Figure 1) (Marelli et al., 2018). When using antitumor viral gene therapy, the administration and distribution of the vectors must be evaluated, taking into consideration their ability to overcome antiviral immune responses and to cross the BBB.
A genetically engineered third generation oncolytic HSV, G47Δ that is armed with IL-12 showed increased survival in a syngeneic murine GBM stem cell model (Cheema et al., 2013). G47Δ was evaluated in a phase II clinical trial in patients with GBM, who received repeated intratumoral stereotactic injections, in addition to TMZ (Todo, 2019).
Newcastle disease virus (NDV) based vectors have a natural tropism for tumor cells, together with oncolytic potential and immuno-stimulatory properties (Schirrmacher et al., 2019). It was shown that the complementary treatment with LaSota strain of the naturally oncolytic NDV induces increased apoptosis in glioma cells, comparing with TMZ alone (Bai et al., 2018). The combination treatment also significantly extended survival in a rat xenograft tumor model (Bai et al., 2018).
Finally, in vivo immunovirotherapy with measles virus (MV) strains in combination with anti-PD-L1 blockade synergistically increased the survival of a murine syngeneic GBM model, together with the enhanced infiltration of activated CD8+ T cells (Hardcastle et al., 2017). MV has already been evaluated in a dose-escalating phase I clinical trial in recurrent GBM in which no dose limiting toxicities were observed (NCT00390299) (Table 3).
reference link: https://www.frontiersin.org/articles/10.3389/fnmol.2021.621831/full
More information: P. Kumthekar el al., “A first-in-human phase 0 clinical study of RNA interference–based spherical nucleic acids in patients with recurrent glioblastoma,” Science Translational Medicine (2021). stm.sciencemag.org/lookup/doi/ … scitranslmed.abb3945



{kind=link}