










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A large-scale new study uncovers which cell types in the human body can be infected by SARS-CoV-2 due to their viral entry factors. The research also suggests that increased gene expression of these viral entry factors in some individuals partially explains the differences of COVID-19 severity reported in relation to age, gender and smoking status.
Reported in Nature Medicine on 2nd March 2021, the study was conducted by researchers from Helmholtz Zentrum München, the Broad Institute of MIT and Harvard, the Wellcome Sanger Institute and University Medical Center Groningen and their collaborators in the Human Cell Atlas Lung Biological Network.
This is part of the Human Cell Atlas* effort to map every cell type in the human body, transforming our understanding of biology and disease.
COVID-19 does not affect everyone in the same way. While the coronavirus, SARS-CoV-2, primarily manifests in the lung, it can infect other organs, too. Clinical observations throughout the pandemic also suggest that some population groups – such as elderly people, men and smokers – tend to be more severely affected by the disease. So far, the molecular reasons for this have not been described.
Previous studies had shown that in order to infect human cells, SARS-CoV-2 needs the cell to contain specific genetic viral entry factors – an ACE2 receptor and a TMPRSS2 or CTSL protease. In this study, researchers from the Human Cell Atlas Lung Biological Network joined forces to contribute and analyse gene expression data from individual cells.
Together, they analysed more than 100 datasets of single-cell gene expression of healthy people, to see which cell types express both ACE2 and a protease.
The analysis showed that specific cell types in the epithelium of the lung and airways, and also in the liver, the colon, and the eye had high expression of the ACE2 receptor and TMPRSS2 protease genes. This means they could potentially be infected with SARS-CoV-2.
The researchers found that these particular cell types from elderly people had higher expression of these entry factors, and that the cells from men had slightly greater expression than from women. In addition, these cells from smokers, in particular airway cells, express more SARS-CoV-2 entry factors than from non-smokers.
These findings match the reported differences in disease severity for COVID-19 patients with age, sex and smoking and offer a molecular explanation for this difference.
“Fighting the pandemic, we cannot rely on conclusions that are limited to only a few observations. Instead, we must rely on robust analysis of big data. For example, to assess whether the ACE2 receptor required for virus entry is more abundant in cells of the elderly population, we need a strong representation of many diverse individuals in our dataset. Using data from the Human Cell Atlas, we could model how genetic viral entry factors in cells are expressed across the population.”
Dr Malte Lücken,computational biologist at Helmholtz Zentrum München and a co-first author of the study
“A key aspect of this large-scale study was the age range of samples we were able to analyse. This study included data from human developmental stages, samples from children and young adults, as well as samples from elderly people. This gave us unique power to assess changes occurring over the human lifetime. The sheer scale of the data allowed us to see molecular differences with age, sex and smoking status.”
Dr Kerstin Meyer, an author on the paper from the Wellcome Sanger Institute
The study investigated which cells are most likely to be infected by SARS-CoV-2. The connection between high expression levels of viral entry factors and increased ease of infection or disease severity has been shown in mice and in the laboratory, but further validation is needed to prove this connection in humans. Other possible factors such as immune system strength were not included in this study.
“This study was the epitome of a whole field coming together. Within the Human Cell Atlas consortium everyone who generated data on the healthy human lung contributed their data, both published and unpublished, to enable our analysis. When we then reached out beyond the consortium, more labs also contributed data to the effort. Only through these contributions was our analysis made possible.”
Professor Fabian Theis, Director of the Institute of Computational Biology at Helmholtz Zentrum München, and Associate Faculty member of the Wellcome Sanger Institute, who coordinated the study
The molecular profile of the cells partially explains how disease severity might differ between population groups, and provides a target for further research. Moving forward, the findings may also help better understand the spread of the coronavirus across the body.
COVID-19 and smoking/vaping
Though there is no direct evidence suggesting the increased susceptibility of smokers/vapers towards COVID-19 infection, various indirect studies prove that this population is at a higher risk to show severe symptoms and need mechanical ventilation as compared to non-smokers.
While analyzing the factors associated with severe disease outcomes in patients admitted to three tertiary hospitals in the Wuhan district, Liu et al (2020), showed that patients with a history of smoking were significantly higher in the progression group (with severe symptoms) than improvement (patients showing recovery) group (27.3% vs 3%) [4]. Again, in Wuhan, the epicenter of the disease in China, the case fatality rates amongst males (2.8%) has been reported to be higher than females (1.7%).
Similar trends have been reported in other hard-hit regions like Italy and Spain, where out of several cases of COVID-19 infection, 58% were men. Furthermore, men are more prone to succumb to the disease with fatalities (72%) [7]. One of the prime reasons for this has been speculated to be higher rate of smoking amongst men (52.1%) than women (2.7%) [8, 9]. Further, smokers are more prone to contract respiratory infections with higher rates of influenza, tuberculosis and pneumonia than non-smokers [9]; which supports the rationale of considering this population group to be at high risk.
Role of epithelial cells and inflammatory response: ACE2 and TMPSSR2
The study of the pathogenesis of COVID-19 points towards the dangers of contracting a disease and eventual complications amongst smokers/vapers due to delayed clearance of virus.
SARS-CoV2 belongs to the family of Coronavirus that obtains its name from the crown-like appearance on imaging. This feature is attributed to a glycosylated cell surface spike (S) protein with two functional domains-S1 and S2. ACE2 has been shown to be the site of host-cell entry for the SARS-CoV2 virus. The S2 domain of the viral spiked envelope has a high affinity to the ACE2 receptor on the lung epithelium.
Interestingly, ACE2 expression has been found to be high amongst smokers (possibly including e-cigarette vapers) and individuals on ACE blockers (patients with hypertension and diabetes), thus rendering them susceptible to the disease [9]. Furthermore, there are more circulating ACE2 in men which provides evidence for gender-based variations in disease severity [10]. ACE2 may be highly expressed in germ cells i.e. more in men vs women.
It is likely that ACE2 is related to nicotinic acetylcholine receptors (nAChRs), particularly alpha7nAChR receptor further supporting that smoking/vaping (nicotine) status might be crucial in the pathophysiology of COVID-19 [11]. The ACE2 receptors (developmentally regulated) are abundant on the lung epithelium, specifically the type II pneumocytes, goblet, nasal epithelial/ciliated and oral mucosal cells [12,13,14].
A recent study has suggested a role of interferon-stimulated response of SARS-CoV-2 entry via ACE2 and TMPSSR2 protease [15]. Studies suggest that ACE2 expression is upregulated in the small airway epithelia of smokers and patients with smoking-associated pathologies like COPD and IPF [15, 16]. Though not tested, vaping (nicotine) may have similar effects, thus making this group more prone to be affected by the disease.
While ACE2 is important for host entry, the host cellular proteases function to activate the viral particle thus facilitating the viral engulfment. In this respect, TMPRSS2 protease is of importance in that ACE2 employs the cellular serine protease TMPRSS2 for S protein priming and host-cell entry [17].
Studies show that the SARS-CoV-2 entry-associated protease, TMPRSS2, is highly expressed in the nasal ciliated and goblet cells. Single cell RNA sequencing analyses of multiple tissues has shown that only a small subset of ACE2+ cells express TMPRSS2, thus suggesting that other proteases might play similar role.
In this respect, Cathepsin B/L has also been shown to be of importance [14]. Interestingly, in vivo and clinical data show that cigarette smoke results in increased expression of Cathepsin B, which raises the possibility of increased susceptibility towards COVID-19 infection amongst smokers [16].
Another cellular protease, furin, cleaves the S1/S2 site of the spike protein of SARS-CoV-2 which is essential for the cell-cell transmission of the virus [18]. Smoking can decrease the effectiveness of serine protease inhibitors (serpins) that control the “furin” activity [19, 20]. Also, evidence suggests that serpin-deficiency attributes to increased viral (Influenza A) susceptibility in C57BL/6 mice [21]. Taken together, these findings point toward increased possibility of COVID-19 contraction amongst smokers/vapers.
Smoking and vaping also affect the tight barrier junction leading to increased epithelial permeability (lung leakiness). In fact, the structural changes due to cigarette smoking including; increased mucosal permeability, impaired muco-ciliary clearance, peribronchiolar inflammation and fibrosis (airway remodeling); could pose little to no resistance towards viral entry amongst smokers as shown in Fig. 1 [22].
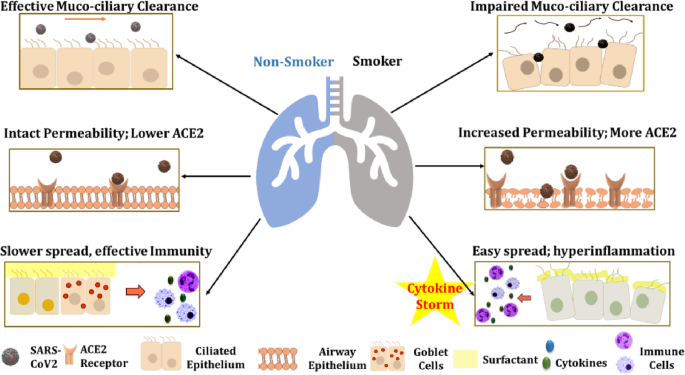
Smoking/vaping causes oxidative stress and inflammatory responses in the lung which make smokers/vapers more susceptible to bacterial/viral infections [23,24,25]. Oxidative stress has adverse effects on the epithelial permeability and ACE2 expression, which may have serious implications in smokers/vapers [26, 27]. ACE2 exists in multiple isoforms with predominance of 90 kDa in the lungs and 120 kDa in kidneys [26].
It can be post-translationally modified by oxidants/carbonyls. Hence ROS generation due to smoking or vaping could adversely affect the ACE2/Angiotensin (1-7) /Mas axis [28]. Likewise, the oxidative stress due to cigarette smoke or e-cig aerosols results in epithelial barrier dysfunction which increases the membrane permeability and susceptibility towards viral/bacterial infections [28,29,30] (Fig. 1).
Covid-19 related genes, such as ACE2 and TMPRSS2 are affected in patients with asthma and are linked with inhaled corticosteroids [31]. This suggests that steroid-resistance seen by smoking in patients with COPD may have ramifications in COVID-19 susceptibility via ACE2 and TMPRSS2.
The most common complication due to SARS-CoV2 infection -Acute respiratory Distress syndrome (ARDS) – is a result of the ‘cytokine storm’ caused due to uncontrolled release of proinflammatory cytokines/chemokines by effector immune cells [32]. These pro-inflammatory mediators include IP-10, MCP-3, HGF, MIG, MIP-1α, IL-6, TNF-α, IFN-γ, IL-2, IL-7 and GM-CSF.
In fact, while studying the transcriptional response towards infection using in vitro model, Blanco-Melo et al. found that SARS-CoV-2 infection in normal human bronchial epithelial cells results in reduced IFN-mediated responses along with heightened production of cytokines/chemokines that enables sustained viral replication [33].
Of interest, the expression of IL-6, TNF-α and other pro-inflammatory cytokines is upregulated in chronic smoking condition and so is the low expression levels of perforin and granzyme B- the two major effector proteins of natural killer (NK) and CD8 T cells [34].
Furthermore, lung autopsy of COVID-19 patients demonstrated neutrophil infiltration in pulmonary capillaries with fibrin deposition and extravasation of neutrophils into the alveolar space [35]. These observations point towards formation of Neutrophil Extracellular Traps (NETs) that may contribute to organ damage, lung remodelling, and mortality in COVID-19 patients.
Evidence suggests that smoking affects neutrophil trafficking, NET formation, humoral and cell-mediated immune responses as shown in Fig. 1. This could eventually lead to susceptibility towards ARDS development further augmenting the disease pathogenesis [35].
In this respect, it is important to mention about the susceptibilities of old smokers/vapers with comorbidities like COPD or IPF. It is known that older patients are more likely to develop pneumonia and respiratory failure due to SARS-CoV-2 infection, which suggests that cellular senescence might play an important role in the disease pathogenesis for COVID-19 [35].
It has been shown that a lowered expression of regulatory proteins like TRIB3 (negative regulator of NF-kappaB signaling) and SIRT1 (anti-aging and anti-inflammatory) amongst aged/older individuals, rendering them more prone to infection [36, 37]. Interestingly, our group showed that the SIRT1 expression is lowered in the lungs of smokers and COPD patients [37].
This highlights the possible involvement of SIRT1 and senescence-associated pathways in modulating SARS-CoV-2 pathogenesis in humans, thereby putting smokers/vapers at a higher risk of contracting an infection. Further, gene tribbles homolog 3 (TRIB3) is decreased during aging in male, and its protein interacts with nucleocapsid protein and RNA dependent polymerase of the virus [36].
The same could be the case with vapers who use e-cigarettes. Considering the rapidly increasing cases of vaping-induced lung pathologies, CDC has coined the term ‘e-cigarette or vaping product use associated lung injury (EVALI)’ to characterize conditions like acute lung injury, acute fibrinous pneumonitis, diffuse alveolar damage, or pneumonia accompanied by bronchiolitis. Such insults increase the possible risk amongst vapers.
In contrast, e-liquid constituents interact with the pulmonary surfactants, i.e. dipalmitoylphosphatidylcholine (DPPC), which could lead to induction of innate immune responses in ENDS users. The lipid dysregulation in the airways of ENDS user could render them more prone to the COVID-19 infection [38]. Furthermore, it is possible that EVALI and COVID-19 have similarities as both develop interstitial pneumonia leading to ARDS [38].
In fact, both EVALI and COVID-19 are characterized by decreased arterial oxygen saturation and bilateral pneumonia, thus making it difficult in detecting the two conditions [39, 40] Also, considering that many people with COVID-19 infection do not show any symptom of the disease, there is a likelihood of the vapers with EVALI being the asymptomatic carriers of COVID-19 [41].
Further, research is required to test the hypothesis that COVID-19 and vaping are associated with severe EVALI. Similar to EVALI, patients with COVID-19 showed elevated levels of several cytokines (CCL2/MCP-1, CXCL10/IP-10, CCL3/MIP-1A, and CCL4/MIP1B) in BALF and peripheral blood mononuclear cells [42].
It is also possible that exosomes/extracellular vesicles released by lung epithelial cells may trap SARS-CoV2 and their respective miRNA/RNA, which would trigger a cytokine storm to other neighboring cells in response to smoking [43]. ACE2 positive cells may play a role in viral entry [44]. Exosomes may be pro-inflammatory or can be exploited pharmacologically in lung diseases [45, 46].
Table 1 Therapeutic options for COVID-19 with respect to lung cytokine storms by COVID-19
From: SARS-CoV-2 COVID-19 susceptibility and lung inflammatory storm by smoking and vaping
| Treatment/ Prophylaxis Options | Rationale | Pros | Cons | Reference |
|---|---|---|---|---|
| Targets from host’s immune system (IL6 blockers: Actemra, Tocilizumab. Monoclonal antibodies: Kevzara-sarilumab) | Preventing excessive inflammatory responses. | Modulation of host’s immunopathological responses would decrease risks of ARDS. | Immune-modulation could have adverse effects | [48] |
| ACE inhibitors (e.g.Umifenovir) | ACE inhibitors may target the S1 domain and ACE2 interaction thus preventing virus entry. | ACE modulation has successfully been employed in treating conditions like hypertension, heart failure and atherosclerosis. | Role of ACE inhibitors in COVID-19 is not clear. | [9, 49] |
| TMPRSS2 inhibitor (e.g.Camostat, Nafamostat) | TMPRSS2 inhibition could prevent the viral activation preventing virus entry. | TMPRSS2 inhibition may have little on-target side effect. | Proteases other than TMPRSS2 (e.g. Cathepsin L, TTSP) might have a role in viral activation. | [50, 51] |
| Chloroquine/Hydroxychloroquine | It could prevent viral entry and have other immune-modulatory effects. | Its anti-inflammatory properties could help monitor immunopathological responses in patients. | It is associated with side effects like nausea, headache, blurred vision, vomiting, cramps, and diarrhea. | [52,53,54] |
| Anti-viral agents (e.g.remdesivir, favipiravir, ripavirin) | They target the viral replication by inhibiting the RNA polymerase enzyme. | These agents have shown promising results during initial clinical trials. | Use of antivirals has the risk of developing resistance amongst some patient populations. | [47, 55] |
| Convalescent Plasma | It involves use of passive antibody therapy to provide viral neutralization. | It can be used for both prophylaxis or treatment. Its efficacy has been tested in previous infections like SARS, Ebola, and hepatitis. | It has a known risk of inadvertent infection due to blood transfer and antibody dependent enhancement of infection (ADE). | [56] |
| Targets from viral structure (like; E protein, Mpro3CLpro, Furin-like cleavage site) | Targeting viral structure would prevent viral host-cell entry and replication. | This method would design SARS-CoV2-specific treatment | Finding a potential cure by this method might take some time before it reaches clinic. | [57,58,59] |
reference link: https://journal-inflammation.biomedcentral.com/articles/10.1186/s12950-020-00250-8
reference link: https://www.sanger.ac.uk/news_item/sars-cov-2-infects-cells-via-specific-viral-entry-factors-that-are-more-abundant-in-elderly-men-and-smokers/



{kind=link}