











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Nearly one in seven Britons who tested positive for COVID-19 continued to have symptoms for at least 12 weeks, according to a UK study released Thursday.
The Office for National Statistics said the study of over 20,000 people who had tested positive from April last year to March this year found 13.7 percent had symptoms that lasted for at least 12 weeks.
This was based on people’s self-reported symptoms of so-called “long COVID”. The list of 13 symptoms included fatigue, muscle pain and difficulty concentrating as well as loss of taste and smell.
Women were more more likely (14.7 percent) to report such long-lasting symptoms than men (12.7 percent).
Those aged 35-49 were most likely to report symptoms at five weeks (25.6 percent).
The study of UK patients was based on a random sample of 21,622 participants who tested positive from swabs and were asked about their symptoms monthly.
A control group who were unlikely to have been infected was also set up. It found they were eight times less likely to have such symptoms.
A larger survey of 1.1 million people self-reported long COVID over the four weeks ending March 6, 2021, the ONS said.
Ben Humberstone, Head of Health Analysis and Life Events at the ONS said this was its first analysis of new data and “our understanding of it and its quality will improve over time”.
Long COVID “is an emerging phenomenon that is not yet fully understood”, he added.
Britain, one of the countries worst hit by the pandemic, has recorded nearly 127,000 deaths from COVID and 4,350,266 cases.
However, the number of daily deaths and positive tests have fallen steadily amid a strong vaccination campaign.
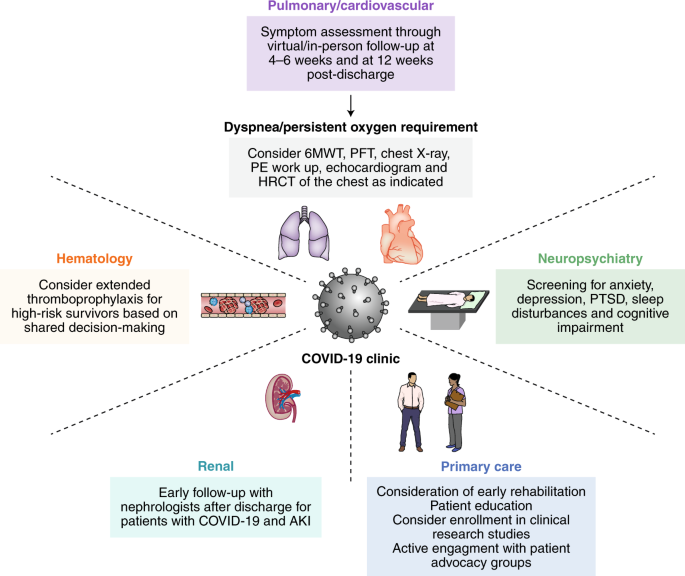
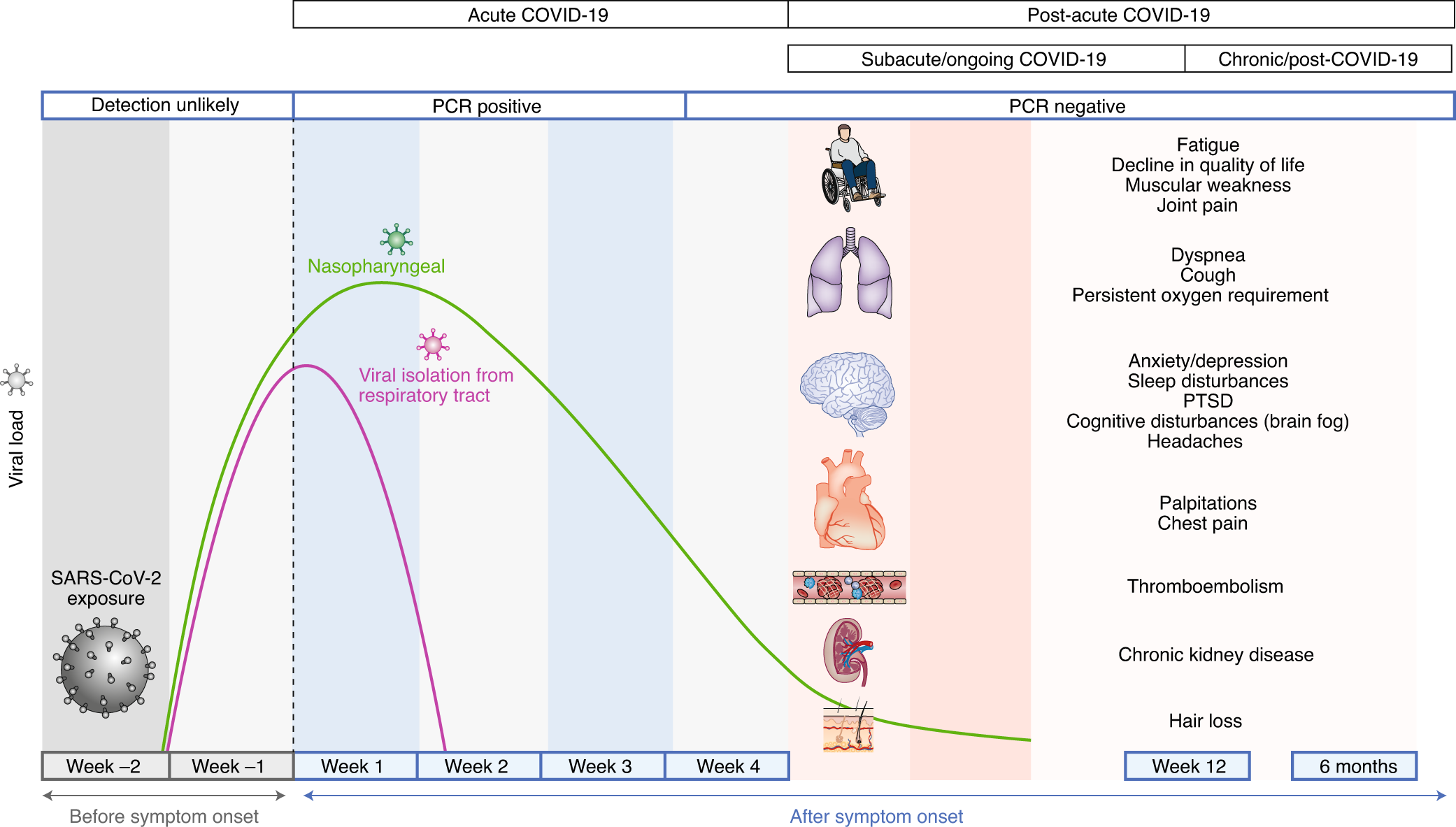
Box 1 Summary of post-acute COVID-19 by organ system
Pulmonary
- Dyspnea, decreased exercise capacity and hypoxia are commonly persistent symptoms and signs
- Reduced diffusion capacity, restrictive pulmonary physiology, and ground-glass opacities and fibrotic changes on imaging have been noted at follow-up of COVID-19 survivors
- Assessment of progression or recovery of pulmonary disease and function may include home pulse oximetry, 6MWTs, PFTs, high-resolution computed tomography of the chest and computed tomography pulmonary angiogram as clinically appropriate
Hematologic
- Thromboembolic events have been noted to be <5% in post-acute COVID-19 in retrospective studies
- The duration of the hyperinflammatory state induced by infection with SARS-CoV-2 is unknown
- Direct oral anticoagulants and low-molecular-weight heparin may be considered for extended thromboprophylaxis after risk–benefit discussion in patients with predisposing risk factors for immobility, persistently elevated D-dimer levels (greater than twice the upper limit of normal) and other high-risk comorbidities such as cancer
Cardiovascular
- Persistent symptoms may include palpitations, dyspnea and chest pain
- Long-term sequelae may include increased cardiometabolic demand, myocardial fibrosis or scarring (detectable via cardiac MRI), arrhythmias, tachycardia and autonomic dysfunction
- Patients with cardiovascular complications during acute infection or those experiencing persistent cardiac symptoms may be monitored with serial clinical, echocardiogram and electrocardiogram follow-up
Neuropsychiatric
- Persistent abnormalities may include fatigue, myalgia, headache, dysautonomia and cognitive impairment (brain fog)
- Anxiety, depression, sleep disturbances and PTSD have been reported in 30–40% of COVID-19 survivors, similar to survivors of other pathogenic coronaviruses
- The pathophysiology of neuropsychiatric complications is mechanistically diverse and entails immune dysregulation, inflammation, microvascular thrombosis, iatrogenic effects of medications and psychosocial impacts of infection
Renal
- Resolution of AKI during acute COVID-19 occurs in the majority of patients; however, reduced eGFR has been reported at 6 months follow-up
- COVAN may be the predominant pattern of renal injury in individuals of African descent
- COVID-19 survivors with persistent impaired renal function may benefit from early and close follow-up in AKI survivor clinics
Endocrine
- Endocrine sequelae may include new or worsening control of existing diabetes mellitus, subacute thyroiditis and bone demineralization
- Patients with newly diagnosed diabetes in the absence of traditional risk factors for type 2 diabetes, suspected hypothalamic–pituitary–adrenal axis suppression or hyperthyroidism should undergo the appropriate laboratory testing and should be referred to endocrinology
Gastrointestinal and hepatobiliary
- Prolonged viral fecal shedding can occur in COVID-19 even after negative nasopharyngeal swab testing
- COVID-19 has the potential to alter the gut microbiome, including enrichment of opportunistic organisms and depletion of beneficial commensals
Dermatologic
- Hair loss is the predominant symptom and has been reported in approximately 20% of COVID-19 survivors
MIS-C
- Diagnostic criteria: <21 years old with fever, elevated inflammatory markers, multiple organ dysfunction, current or recent SARS-CoV-2 infection and exclusion of other plausible diagnoses
- Typically affects children >7 years and disproportionately of African, Afro-Caribbean or Hispanic origin
- Cardiovascular (coronary artery aneurysm) and neurologic (headache, encephalopathy, stroke and seizure) complications can occur
The first case of COVID-19 was reported in Wuhan, China, in December 2019.1 COVID-19 is caused by a novel coronavirus, named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or 2019-nCoV). As of 15 November 2020, more than 54 million people have been infected, and more than one million deaths have been reported.2
In Oman, as of 15 November 2020, 118 000 cases have been reported, with 1338 deaths.2 The first two cases were diagnosed on 24 February 2020, in Muscat governorate.3 The acute presentation of a COVID-19 infected patient has been well described in various studies.4
The majority of patients presented with a fever, sore throat, cough, shortness of breath, and chest pain. Many papers have described multi-organ involvement.5 The acute illness is mild in the majority of the patients. Even so, around 20% of those infected need hospitalization, and around 5% require critical care with non-invasive or mechanical ventilation.6
There is a misconception that all patients with COVID-19 may recover within two weeks; this is not always the case. The long-term consequences of COVID-19 infection are not well understood. In addition, prolonged recovery of symptoms has been described even in patients who had mild symptoms and did not require hospitalization.7,8
This manifestation was termed post-acute COVID-19 syndrome or ‘long COVID’.9 This editorial aims to explore post-acute COVID-19 syndrome or long COVID.
There is no clear definition of post-acute COVID-19 syndrome. In general, it is an illness described among patients who have recovered from COVID-19 but still have ongoing symptoms or among those who continued to have symptoms for longer than normally expected.10 Some authors have suggested the presence of symptoms beyond 12 weeks from the onset of illness as a description of post-acute COVID-19 syndrome.9
Other studies have divided these patients into three groups: those who had severe manifestations such as acute respiratory distress syndrome (ARDS), requiring intensive care unit (ICU) admission; those who were not admitted during the acute illness but later presented with symptoms and signs of end-organ damage, such as cardiac or respiratory disease; and those who did not require hospitalization but presented with prolonged symptoms without evidence of end-organ damage.11 It is interesting to note that post-acute COVID-19 syndrome is more common in women.
The exact mechanism of this post-COVID-19 presentation is obscure. Previous investigators suggested low antibody response to SARS-CoV-2 infection, prolonged inflammatory response to the SARS-CoV-2 infection, deconditioning, and re-infection with SARS-CoV-2 as possible mechanisms that might explain post-COVID-19 presentation.7
There is a marked variation in the presentation of post-acute COVID-19 syndrome. Patients may present with non-specific symptoms such as fatigue, muscle aches and pains, poor sleep, cough, and breathlessness, to more specific organ-related symptoms, such as orthopnea, leg swelling, and exercise intolerance due to COVID-19 induced heart failure.7 Furthermore, chest pain and significant breathlessness might be due to pulmonary embolism.12 Autonomic symptoms such as palpitations with mild exertion, night sweats, and poor temperature control were also described.12 The symptoms might be cyclical in some patients.8
Based on our experience of following-up COVID-19 patients discharged from the hospital, fatigue appears as a prominent feature, even at 12 weeks post-discharge. Patients assert that they were unable to return to their baseline activity level. They find trivial daily activities fatigue-inducing. This is a major complaint that has been acknowledged by the literature.4 Another prominent feature of long COVID experienced by our patients is shortness of breath.
This was more significant among patients with severe COVID-19 who were admitted to ICU and required either non-invasive or mechanical ventilation. Further investigation revealed mild anemia in some patients, evidence of pulmonary embolism in some, and changes suggestive of pulmonary fibrosis in computer tomography of the chest among others.
Cardiac causes such as heart failure with preserved ejection fraction or impaired ventricular function were found in a small number of patients. However, there was no cause identifiable in the majority of patients.
Post-acute COVID-19 syndrome management remains a clinical challenge as there are no evidence-based international guidelines to follow at the time of writing. Pulmonary embolism is managed in the usual way with anticoagulation for at least three months.
There is no consensus on the benefit, or duration, of prolonged prophylaxis, with low molecular weight heparin, post-discharge. Management of post-COVID-19 pulmonary fibrosis is also unclear. Clinical, radiological, and biochemical markers are required to help clinicians anticipate which patients with COVID-19-related ARDS are susceptible to developing pulmonary fibrosis following the resolution of COVID-19.13 We have used systemic steroids in some patients with good results. The role of the antifibrotic drugs, pirfenidone and nintedanib, is awaiting clinical trial evidence.
A unified definition of long COVID and characterization of its manifestation are important for early detection. In addition, more research should be directed to identify risk factors and exact mechanisms leading to the development of long COVID syndrome. Such knowledge may enhance further research aimed at the prevention of such a complication.
In conclusion, a large number of patients have been affected by COVID-19, and as physicians, we are going to face many patients with symptoms suggestive of long COVID. The entire spectrum of long COVID is not well characterized. Further research looking at risk factors, mechanisms explaining development of long COVID, and preventative measures are imperative to prevent such a complication.
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7838343/



{kind=link}