










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



In a new study, researchers identify three clinical COVID-19 phenotypes, reflecting patient populations with different comorbidities, complications and clinical outcomes. The three phenotypes are described in a paper published this week in the open-access journal PLOS ONE 1st authors Elizabeth Lusczek and Nicholas Ingraham of University of Minnesota Medical School, US, and colleagues.
COVID-19 has infected more than 18 million people and led to more than 700,000 deaths around the world. Emergency department presentation varies widely, suggesting that distinct clinical phenotypes exist and, importantly, that these distinct phenotypic presentations may respond differently to treatment.
In the new study, researchers analyzed electronic health records (EHRs) from 14 hospitals in the midwestern United States and from 60 primary care clinics in the state of Minnesota.
Data were available for 7,538 patients with PCR-confirmed COVID-19 between March 7 and August 25, 2020; 1,022 of these patients required hospital admission and were included in the study. Data on each patient included comorbidities, medications, lab values, clinic visits, hospital admission information, and patient demographics.
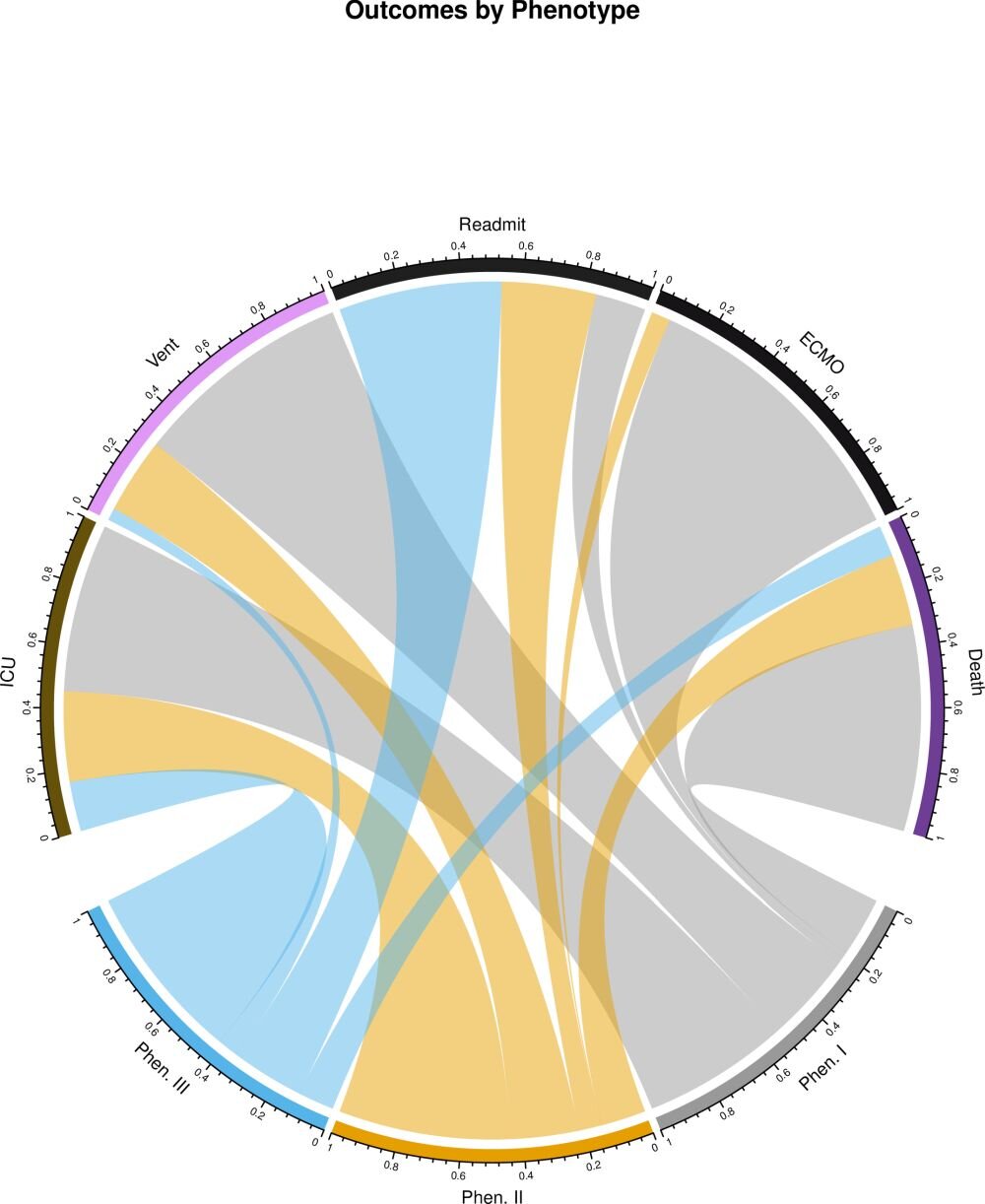
Most patients included in the study (613 patients, or 60 percent) presented with what the researchers dubbed “phenotype II.” 236 patients (23.1 percent) presented with “phenotype I,” or the “Adverse phenotype,” which was associated with the worst clinical outcomes; these patients had the highest level of hematologic, renal and cardiac comorbidities (all p<0.001) and were more likely to be non-White and non-English speaking. 173 patients (16.9 percent) presented with “phenotype III,” or the “Favorable phenotype,” which was associated with the best clinical outcomes; surprisingly, despite having the lowest complication rate and mortality, patients in this group had the highest rate of respiratory comorbidities (p=0.002) as well as a 10 percent greater risk of hospital readmission compared to the other phenotypes.
Overall, phenotypes I and II were associated with 7.30-fold (95% CI 3.11-17.17, p<0.001) and 2.57-fold (95% CI 1.10-6.00, p=0.03) increases in hazard of death relative to phenotype III.
The authors add: “Patients do not suffer from COVID-19 in a uniform matter. By identifying similarly affected groups, we not only improve our understanding of the disease process, but this enables us to precisely target future interventions to the highest risk patients.”
Covid-19 pneumonia is not a straightforward disease. Chest computed tomography (CT) scans can show different versions. There is no single pattern or cluster of clinical presentations.
“Although the pulmonary pattern of critically ill patients with Covid-19 has been defined as acute respiratory distress syndrome (ARDS), it does not always represent or even resemble ARDS,” said Chiara Robba, a professor of neurology, and her colleagues at the University of Genoa.
ARDS is driven by widespread inflammation in the lungs. Fluid accumulates inside air sacs, which hampers gas exchange. Less oxygen enters the blood, depriving organs of oxygen. Its mortality rate hovers at around 40%.
The L and H Phenotypes
In April editorial in Intensive Care Medicine, Professor Luciano Gattinoni — who has been studying ARDS for decades — and his colleagues at the Medical University of Göttingen were the first to suggest that Covid-19 pneumonia has two distinct phenotypes.
- L phenotype: Low elastance (almost normal gas levels in the lungs), low ventilation to perfusion ratio (leading to hypoxemia), low lung weight, and low lung recruitability (low amount of non-aerated tissues).
- H phenotype (similar to severe ARDS): High elastance (low gas levels in the lungs), high right-to-left shunt (heart abnormality), high lung weight, and high lung recruitability (high amount of non-aerated tissues).

L phenotype is the less severe one and may either improve or transition to H phenotype. H phenotype is similar to severe ARDS and occurs about 20–30% of the time, based on their clinical case series, Professor Gattinoni noted. As follows, H phenotype (and not L) should be treated according to the standard protocol for ARDS.
The Revised 3 Phenotypes
Later in May, Professor Robba et al. added another phenotype, and now three phenotypes of Covid-19 pneumonia exist. His paper, “Distinct phenotypes require distinct respiratory management strategies in severe COVID-19,” is published in Respiratory Physiology & Neurobiology.
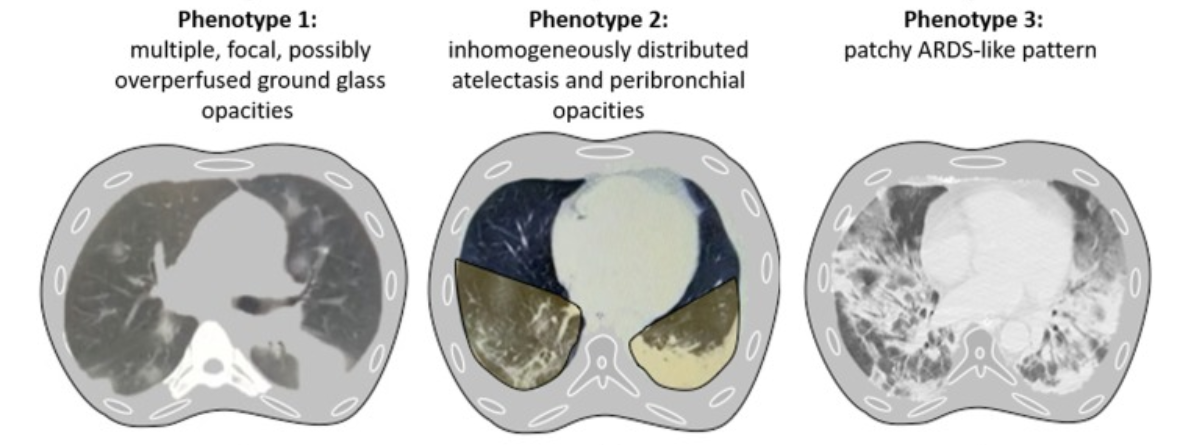
In the image, CT phenotypes 1 and 3 are compatible with the L and H phenotypes proposed by Professor Gattinoni, respectively. The new CT phenotype 2 is the transition phase between the other two.
Because each phenotype has different pathophysiology (patho = disease), treatment strategies need to be catered to each phenotype, they emphasized.
- PEEP ventilation is the primary treatment for each phenotype, though ventilator settings vary for each.
- CT Phenotype 1: Patients have hypoxemia (i.e., a condition of deficient levels of oxygen in the blood). Inhaled nitric oxide (i.e., a pulmonary vasodilator technique) might help. Prone positioning and recruitment manoeuvres (i.e., a technique to open collapsed areas of the lungs and keep them open) are often ineffective.
- CT Phenotype 2: Patients have atelectasis (i.e., a condition of a blocked airway that compromises gas exchange and breathing) and lung derecruitment (i.e., a condition wherein areas of the lung collapsed and lung tissues became poorly aerated). Recruitment manoeuvres might help, whereas inhaled nitrogen oxide therapy is less effective. Prone positing is most effective for this phenotype.
- CT Phenotype 3: Patients have moderate-to-severe ARDs. Prone positioning, recruitment manoeuvres, or ECMO ventilation are last-resort treatments if PEEP ventilation failed.
Extra: Phenotype vs Endotype
Endotype refers to the subtypes of a disease. Covid-19 may have pneumonia, endothelial, or neurological endotypes, for example. Within the pneumonia endotype, there can be many characteristics or traits called phenotypes, such as the L and H.
Similarly, within the neurological endotype called Neuro-COVID, there are three different phenotypes: Cerebral thrombosis with hemorrhagic infarction, demyelinating lesions, and encephalopathy.
Phenotype-based Treatment
Employing different treatment strategies for individual phenotypes of Covid-19 pneumonia is key to recovery, as the professors emphasized. Incompatible treatments might end up worsening disease prognosis.
Take proning, for instance. “We do not recommend prone positioning of Covid-19 patients with phenotype 1,” Professor Robba cautioned. “It should be reserved for phenotypes 2 and 3, to redistribute pulmonary blood flow and reduce atelectasis.”
Further, in L phenotype (or phenotype 1), “patients should be left “quiet”; avoiding doing too much is of a higher benefit than intervening at any cost,” Professor Gattinoni advised. “Understanding the correct pathophysiology is crucial to establishing the basis for appropriate treatment,” he wrote.
More information: Elizabeth R. Lusczek et al, Characterizing COVID-19 clinical phenotypes and associated comorbidities and complication profiles, PLOS ONE (2021). DOI: 10.1371/journal.pone.0248956



{kind=link}