











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Scientists from Hokkaido University have shown that an antigen-based test for quantifying SARS-CoV-2 in saliva samples is simple, rapid, and more conducive for mass-screening.
More than a year into the COVID-19 pandemic, the RT-PCR test remains the gold standard for detection of the SARS-CoV-2 virus. This method requires trained personnel at every step, from collection of nasopharyngeal swab (NPS) samples to interpretation of the results; in addition, the entire process ranges from 24–48 hours on average.
As the virus can be transmitted by an infected person before symptoms develop, and is even transmitted by individuals who are asymptomatic, the ability to screen a large number of people quickly is vital to controlling and preventing the spread of the pandemic.
Faster methods to detect the SARS-CoV-2 antigens have been developed, but they are not as sensitive as the RT-PCR test. In June 2020, a novel antigen-based kit, Lumipulse SARS-CoV-2 Ag kit (Lumipulse), was developed by Fujirebio to quantitatively measure the viral antigen in biological samples within 35 minutes.
A team of scientists from Hokkaido University have used the antigen kit to detect SARS-CoV-2 in saliva samples, and have assessed the efficiency and accuracy of the test compared to RT-PCR. Their findings show that the antigen detection kit, which is used to perform chemiluminescent enzyme immunoassay (CLEIA), can rapidly detect SARS-CoV-2 with good accuracy in these samples. The study was published in the journal The Lancet Microbe.
The scientists tested 2056 individuals from three cohorts: patients with clinically confirmed COVID-19, individuals who had contacted patients with COVID-19, and individuals tested on arrival at Tokyo and Kansai International Airports.
The benefit of using saliva samples is the ease of collection: it is quick and can be collected by the individuals being tested, reducing the risk that healthcare workers are exposed to the virus. Furthermore, self-collection of saliva allows multiple samples to be collected simultaneously for expeditious screening of visitors at large gatherings.
Discussion
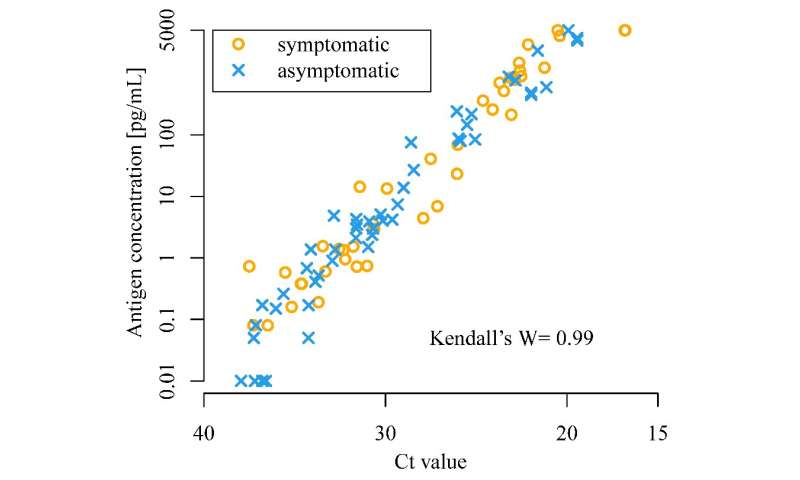
Our results showed high correlation between antigen concentrations measured by CLEIA and RNA load measured by RT-qPCR, indicating CLEIA to be a reliable and accurate test. Improved diagnostic accuracy can be attained if the two tests are used in combination. Accordingly, CLEIA has been in use across Japanese airports as part of a two-step strategy with NAAT since July, 2020.
Quantitative CLEIA could allow for positive and negative thresholds to be adjusted according to estimated prevalence in a local population, and would provide a pretest estimate on the number of RT-qPCR tests that might be necessary for final diagnosis. We found that a cutoff value of 4·00 pg/mL would give 100·0% specificity (CLEIA[–]|RT-qPCR[–]), but with a lower sensitivity of 85·4% (CLEIA[+]|RT-qPCR[+]).
If the diagnosis must be made by CLEIA alone with one cutoff, a low value, such as 0·67 pg/mL, should be used to minimise the compromise in sensitivity while maintaining a specificity greater than 99%, to avoid the isolation of non-infected individuals due to false-positive results. Conversely, if capacity is sufficient to implement RT-qPCR as a confirmatory test after initial testing by CLEIA, a lower threshold, such as 0·19 pg/mL, should be set to increase the sensitivity of CLEIA and its suitability for screening purposes.
For example, assuming a situation in which 100 000 people might be tested with an estimated prevalence of 10%, 10 000 people will be positive by RT-qPCR. In this scenario, applying the most accurate cutoffs for positivity (4·00 pg/mL) and negativity (0·19 pg/mL), 5281 people (10 000 × 47/89; table) will test positive in an initial CLEIA test, with another 3258 patients having an indeterminate CLEIA result and testing positive by NAAT. Of the 90 000 people with RT-qPCR negativity, 7824 people will test negative by NAAT after an indeterminate result from CLEIA. By employing a two-step strategy, NAAT would only be needed in 11 082 of 100 000 people (ie, about 11% of all individuals).
At an estimated prevalence of 50%, a similar calculation shows that the number of people who would require confirmation by NAAT to be 20 639 (∼21%). Therefore, this two-step testing strategy exploits the advantage of rapid and accurate quantitative antigen testing to save the resources for NAAT to approximately 10–20% of an entire test population.
Previous reports on the Lumipulse G SARS-CoV-2 Ag assay in NPS samples showed a concordance with RT-qPCR of 91·4% in 313 samples15 and 98·2% in 548 samples.16 By contrast, Kobayashi and colleagues17 reported a lower concordance of 66·0% in 100 NPS samples, although samples with discrepant results were collected considerably later in the course of infection than those with concordant results. To our knowledge, our study is the first to evaluate saliva samples with CLEIA.
In addition, we obtained specimens from more than 2000 symptomatic and asymptomatic people, and found 98·2% (2020 of 2056 samples) of CLEIA results to be in agreement with results by RT-qPCR. All samples were collected prospectively and consecutively, providing credibility to our results, with the implication that CLEIA might be a viable alternative to RT-qPCR.
Furthermore, all tests were done with self-collected saliva, enabling simultaneous parallel sample collection and rapid processing, which are in need at sites of mass screening. Despite use of a central laboratory to ensure quality control in this study, the size of the automated machine (Lumipulse G1200; 1·20 m × 0·80 m × 1·45 m) is small enough to be installed at points of care.
A positive RT-qPCR result does not necessarily indicate presence of live virus,22 and studies in the past year have shown COVID-19 patients with Ct values greater than 33 or 34 on RT-qPCR not to be contagious.23, 24 Conversely, in our study, 15 (0·7%) of 2056 samples had antigen concentrations between 0·67 pg/mL and 4·00 pg/mL but were negative on RT-qPCR. This discrepancy could reflect a false-positive CLEIA, but the possibility of a false-negative RT-qPCR result cannot be ruled out, and the clinical implication of this discrepancy remain to be elucidated.
Large-scale comparative studies in recent months have shown that saliva and NPS samples have equivalent efficacy in the detection of SARS-CoV-2 by RT-qPCR.9, 10, 11, 12 Since saliva testing has substantial logistic advantages over NPS testing, we are confident that a combination of CLEIA and NAAT with self-collected saliva is the best available testing method for mass screening of SARS-CoV-2.
Reverse transcriptase loop-mediated isothermal amplification (LAMP)25 has become the second most common NAAT after RT-qPCR with several advantages over RT-qPCR, including rapid turnaround time within 30 min, ease of implementation, and potential utility at the point of care with a simple device.11, 14, 26, 27, 28, 29, 30, 31 In 2020 we reported that LAMP had equivalent efficacy to RT-qPCR in detecting SAR-CoV-2 when testing saliva from asymptomatic people in our contact tracing and airport quarantine cohorts.11 For these reasons, LAMP is currently being used at the international airport quarantine stations in Japan as the confirmatory NAAT test after indeterminate results from CLEIA.
Limitations of this study include the absence of longitudinal clinical follow-up and the low number of positive cases in the airport quarantine cohort. We were unable to confirm whether the participants who tested negative did not subsequently develop COVID-19. However, simple follow-up might be inadequate as a large number of false-negative people might never develop symptoms and yet be infectious (although a low viral load might attenuate transmission23).
Therefore, negative test results might warrant repeated testing in individuals with strongly suspected infection, such as people travelling from countries with high prevalence of COVID-19 or people consistently in close contact with known infected patients. In the present study, we showed that test specificity with CLEIA was 99·8% or greater if the higher cutoff was set to 2·43 pg/mL, as the highest concentration in the 1967 specimens that tested negative on RT-qPCR. Considering the differences between the specificities of CLEIA and RT-qPCR, a higher CLEIA positivity cutoff would be necessary if the greatest priority is minimising false-positives.
In summary, we showed CLEIA to be a reliable alternative to RT-qPCR with high concordance between the results of the two tests in a large population. Furthermore, use of these tests in a stepwise strategy with self-collected saliva is more efficient than use of NPS and RT-qPCR alone in real-life mass screening settings. A two-step testing methodology with CLEIA and LAMP has already been implemented at Japanese airport quarantine stations, facilitating expeditious processing of samples from international travellers, with all tests done at the point of care.
We believe that the two-step test strategy with self-collected saliva is presently the most effective method for screening large numbers of people in a short period. Further studies on prospectively validating the two-step approach and data on longitudinal follow-up after point-of-care testing might be warranted.
reference link : https://www.sciencedirect.com/science/article/pii/S2666524721000926
More information: Isao Yokota et al, A novel strategy for SARS-CoV-2 mass screening with quantitative antigen testing of saliva: a diagnostic accuracy study, The Lancet Microbe (2021). DOI: 10.1016/S2666-5247(21)00092-6



{kind=link}