











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The new research published in eNeuro highlights a need to develop safer types of painkillers for pregnant women.
Opioids like oxycodone are prescribed to pregnant women to treat pain, but the drugs may affect the fetus, too. Opioids can pass through the placenta, binding to receptors in the fetal brain, which can lead to opioid withdrawal in newborn babies.
The long-term consequences of prenatal opioid exposure haven’t been fully studied, however.
To explore this, Martin et al. administered oxycodone to female mice every day for the two weeks prior to and throughout the duration of their pregnancy.
The team administered a range of behavioral tests on the offspring during weaning and later in adulthood. The offspring exposed to oxycodone during gestation showed signs of impaired social behaviors and communication. They were also larger and less active than the control mice.
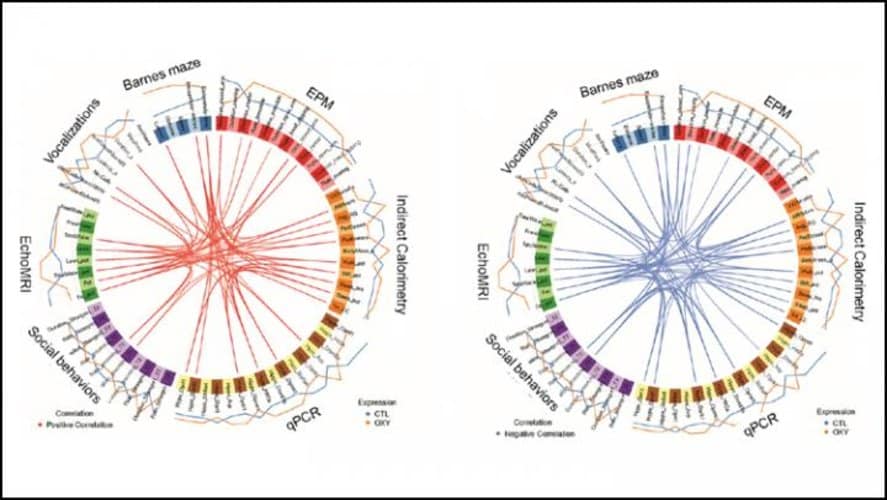
The research team examined the gene expression of opioid receptors in the offspring. In the hippocampus, a region involved in learning and memory, one type of receptor increased in male mice while a different receptor decreased in female mice.
These results reveal prenatal opioid exposure can have lifelong effects on offspring.
Pregnancy
Since 2002, the incidence of first time heroin use has doubled among women and among young adults aged 18–25 years, a demographic that includes many pregnant women.33 According to the American College of Obstetrics and Gynecology, 1% of pregnant women report nonmedical use of opioid pain medications.34
Pregnant women with opioid use disorder are at increased risk for adverse pregnancy outcomes including preterm labor, fetal death, growth restriction, and neonatal abstinence syndrome, which increased by 300% from 2000 to 2009.35,36
Universal screening for substance use disorders, including opioid use disorder, is recommended in pregnancy, and should occur at the initial prenatal visit and be performed again once per trimester for those who screen positive for past use. This should be done using a validated screening tool such as the 4Ps Plus questionnaire (see Figure 1),37 an instrument to quickly identify obstetric patients at risk for misusing alcohol, tobacco, and illicit drugs, or the three question set of “In the past year how many times have you had more than four alcoholic drinks per day, used tobacco, or taken illegal drugs or used prescription drugs for non-medical purposes?”.38
Screening by means of a questionnaire is recommended over the use of universal urine drug screens, which have poor sensitivity and specificity for chronic use, and it is essential that the topic of substance use disorder be broached in a non-judgmental fashion. Care for women with opioid use disorder should be approached in a manner similar to that for women with other chronic conditions such as diabetes, chronic hypertension, obesity, or any of the myriad of maternal comorbidities that complicate pregnancy.

The goal of treating maternal OUD is to use the lowest possible dose of methadone or buprenorphine in order to eliminate cravings and withdrawal. While it has traditionally been taught that maternal withdrawal during opioid detoxification is harmful to the fetus, a recent publication by Bell, et al. challenges this notion.39
Patients will frequently state a desire to wean off of MAT during pregnancy in order to minimize the risk of neonatal abstinence syndrome (NAS). We generally recommend against this approach due to the unacceptably high risk of relapse, which ranges from 35 to 75% depending on the intensity of outpatient therapy.
In regards to the fetus, maternal opioid use disorder carries significant risks. Maternal overdose and the associated risk of coma, aspiration, hypothermia, and cardiovascular collapse can be life threatening for the developing fetus. Neonates exposed to opioids in utero have a risk of neonatal abstinence syndrome (NAS) that is as high as 90%.34 NAS is characterized by neonatal irritability, temperature dysregulation, poor feeding, failure to thrive, and in some cases seizures.
This condition may last for up to 10 weeks after delivery and may necessitate a prolonged NICU admission.40 Some data suggests a lower rate of NAS with buprenorphine therapy as opposed to methadone, but this data is far from conclusive.41 Although buprenorphine alone (SubutexTM) has been traditionally preferred over buprenorphine-naloxone (SuboxoneTM) for pregnant women due to concerns about the fetal effects of naloxone, oral naloxone is biologically inert and a growing body of data supports the safety of buprenorphine-naloxone use in pregnancy.
The peripartum period is a particularly challenging time to provide care for women with OUD. Due to chronic opioid use and the development of tolerance, these individuals may require larger doses of pain medications than providers are typically accustomed to giving. This can lead to the patient being accused of ‘drug seeking behavior’ and her pain going untreated.
Our approach to caring for women on MAT at the time of delivery is to maximize the use of multimodal analgesia and to use regional anesthesia whenever possible. Neuraxial anesthesia (i.e., spinal or epidural) is the preferred method for both vaginal and cesarean delivery. Of note, there is no contraindication to intrathecal morphine in the setting of MAT use.
In women with OUD undergoing vaginal delivery, we also treat pain with acetaminophen and NSAIDS and if necessary increase the dose of methadone or buprenorphine. In women who continue to have refractory pain, we will use adjunctive opioid therapy in the form of oral medication or patient controlled analgesia (PCA) as appropriate (intravenous or transdermal fentanyl in the setting of buprenorphine use) with early outpatient follow up with the patient’s MAT provider.
Pregnant women on MAT with buprenorphine and methadone require careful attention in regards to medication interactions. The use of opioid agonist/antagonists such as butorphanol (Stadol™) or nalbuphine (Nubain™) is absolutely contraindicated in patients on methadone or buprenorphine due to the risk of precipitated withdrawal. Additionally, our practice is to avoid the concurrent use of full opioid agonists with buprenorphine.
Because of buprenorphine’s higher binding affinity for the mu receptor compared with full agonists (except fentanyl),42 individuals undergoing induction of buprenorphine therapy must be free of opioids and in withdrawal before starting buprenorphine. In an individual with opioid dependence who has a full opioid agonist in her system and is therefore not in withdrawal, giving a dose of buprenorphine will result in the partial agonist buprenorphine displacing the full agonist from the mu receptors, which would in turn precipitate withdrawal due to the lower mu agonist activity of buprenorphine.
Furthermore, an individual on long term buprenorphine therapy with refractory pain is unlikely to achieve adequate analgesia with typical mu receptor agonists (oxycodone, hydrocodone, morphine, etc) because large doses of these medications will be necessary to overcome the higher binding affinity of the buprenorphine.
As part of the treatment plan, it is essential to assure patients that the care team will do everything possible to manage the pain associated with labor and delivery and that the treatment of surgical pain will not increase the risk of relapse. If a patient enters prenatal care on MAT, it is recommended that the same provider continue to manage her MAT during pregnancy.
In cases where MAT is initiated by an obstetric provider, arrangements should be made for continued treatment with MAT post-partum, which may entail cooperation with a methadone clinic, primary care provider, or addiction psychiatrist as appropriate. It is also important to arrange for consultation between the patient and the pediatricians or neonatologists who will be caring for the baby after delivery. The care of the child affected by maternal opioid use does not end at delivery and the patient should have an opportunity to ask questions regarding the post-partum care plan.
Although MAT with either methadone or buprenorphine is recognized as the standard of care for treating OUD during pregnancy, significant barriers to care exist and prevent more than half of pregnant women with OUD from receiving the recommended treatments.43
Many women with OUD live in states where methadone is not covered under Medicaid, or live in areas where there are no physicians who are licensed to prescribe buprenorphine. Women in the criminal justice system are even less likely to receive standardized care for OUD. In addition to issues relating to accessibility and funding, women are significantly less likely to receive MAT (or even to seek prenatal care at all) in states that permit child abuse charges for illicit drug use during pregnancy.
Although Tennessee is currently the only state in which a woman can face criminal charges for substance abuse during pregnancy, 18 states permit civil child abuse charges that may result in termination of parental rights. Missouri has no such laws and does not require drug testing or physician reporting of suspected substance use disorders during pregnancy.28 Missouri is also one of only 12 states that offers pregnant women priority access to treatment programs for substance use disorders and does not impose limits on the dose or duration of buprenorphine therapy.
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6140233/
Original Research:“Maternal Oxycodone Treatment Results in Neurobehavioral Disruptions in Mice Offspring” by Rachel E. Martin, Madison T. Green, Jessica A. Kinkade, Robert R. Schmidt, Tess E. Willemse, A. Katrin Schenk, Jiude Mao and Cheryl S. Rosenfeld. eNeuro



{kind=link}