











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Researchers have long suspected that the symptomology of schizophrenia fundamentally arises from disrupted synaptic function, or abnormalities in the way that neurons communicate with one another, perhaps leading to an imbalance between excitatory and inhibitory transmission.
The authors, led by Rick Adams, Ph.D., at University College London, used electroencephalography (EEG), a noninvasive technique that measures brain waves, to collect data from 107 participants with a diagnosis of schizophrenia, 57 of their relatives and 108 control participants. The EEGs of people with schizophrenia displayed hallmark signs including increased theta waves.
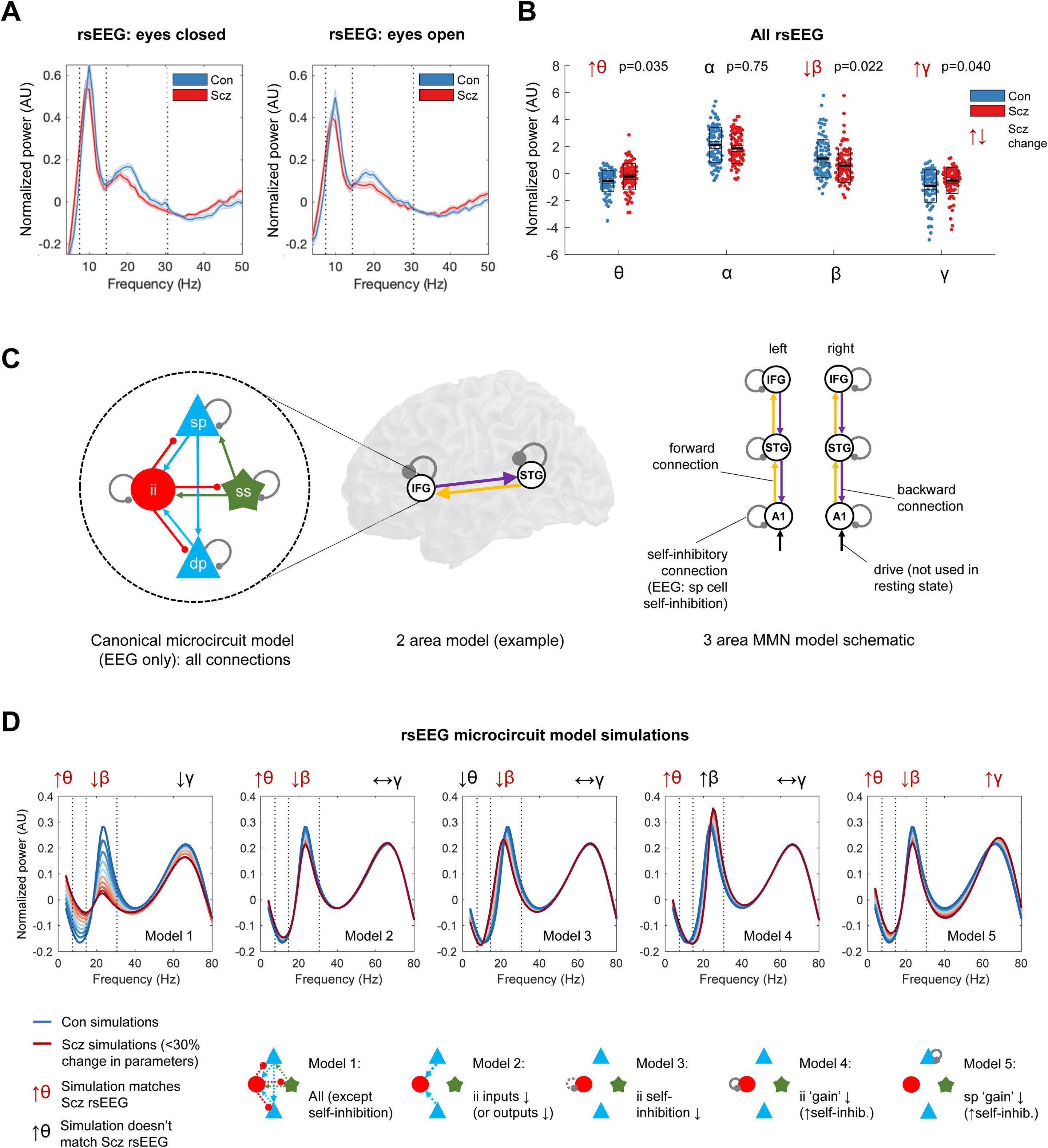
To find out, Dr. Adams and colleagues used computational modeling of the EEG data, which showed that the EEG differences seen in people diagnosed with schizophrenia resulted from decreased synaptic gain.
This means that excitatory neurons had a diminished ability to stimulate one another. Symptoms of schizophrenia including auditory hallucinations, however, were associated with a loss of neural inhibition, especially in auditory brain areas.
“This might mean that the loss of excitation comes first, and the brain tries to compensate for this by reducing inhibition, but then this leads to hallucinations,” Dr. Adams said.
“Imagine you are trying to listen to someone speaking on the radio, but the signal is very weak; if you turn the volume up, the speech is louder–but so is all the static and background noise–and so you may mistake some of this noise for actual speech. Something analogous might be happening in brain circuits in schizophrenia.”
John Krystal, MD, Editor of Biological Psychiatry, said of the work: “Working out the fundamental features of synaptic dysfunction in schizophrenia may help to guide both pharmacological and neurostimulation treatments for this disorder.”
Auditory verbal hallucinations (AVH) are vivid perceptions of sound that occur without corresponding external stimuli and have a strong sense of reality. It occurs in 60–80% of schizophrenia patients (1) and causes multiple dysfunctions and poor control of behaviors (2, 3). Schizophrenia patients with AVH may have an increased tendency toward violent behaviors or acts (4–6), which may pose a threat and serious burden to society and their families.
Controlling and eliminating symptoms of hearing voices is difficult in treatment. Many efforts have been devoted to the treatment of auditory hallucinations, but the results still remain unsatisfactory (7). Studies have been conducted to investigate the efficacy of antipsychotic medications for AVH in schizophrenia patients, which exhibited a significant treatment effect of several typical and atypical antipsychotics (8, 9).
However, there are still a considerable minority of schizophrenia patients showing no treatment effect of antipsychotics (9) and AVH can be drug-resistant and become chronic in around 25% of schizophrenia patients (10). Brain stimulation and psychological intervention are also applied in the treatment for AVH, but the curative effect is not ideal.
For example, transcranial magnetic stimulation may reduce the frequency and severity of AVH, but the efficacy effect size of 1 Hz transcranial magnetic stimulation was just 0.44, supported by meta-analysis (11). And cognitive-behavioral therapy, which is considered as the most investigated psychological intervention of AVH, has an average effect size of 0.44 (12).
Schizophrenia patients experiencing AVH usually report that they have been hearing words, sentences and conversations which often comment on their thoughts. Healthy individuals who experience this are typically aware that the “voices” they hear are false perceptions and originate from their mind.
In addition, they seem to be able to cope with this false perceptual experience by recruiting inhibitory control functions. However, hallucinating schizophrenia patients seem to focus on “voices” and appear less able to exhibit inhibitory control and thus are less able to attend to events around them (13).
It is suggested that inhibitory top-down control functions should play an essential role in modulating experience of voice that originates from one’s mind or an external source. In other words, deficits in inhibitory top-down control process may be important in AVH (14).
Neuroimaging studies have shown that AVH results from a variety of alterations in brain structure (15, 16). Findings of structural imaging studies converge on gray matter reductions in the superior temporal gyrus, insula and inferior frontal gyrus as well as abnormalities in the connecting white matter between these regions, which associated with the processing of auditory verbal stimuli and executive control functions.
Paulik et al. conducted a study with 589 undergraduate students who were drawn into high- and low-predisposed groups using the Launay-Slade Hallucination Scale (LSHS). They found that compared with the low LSHS group, the high LSHS group showed significantly increased false alarms on critical “inhibitory” runs (17).
And according to Waters et al. and Badcock et al., the damage level of inhibitory control ability was positively correlated with the auditory hallucination severity (18, 19).
Electrophysiological approaches also provide important insights into the underlying mechanisms of AVH. Especially the event-related potentials (ERP), which are real-time measures of neural activity with high temporal resolution and promising tools to explore brain dynamics that underlie deficits during task performance.
ERP recordings in schizophrenia with AVH have shown deficits in a series of components, including the early, P50 (20) and mismatch negativity (21) and the later, P3. P3 is a measure of inhibitory control, which has been well-studied in schizophrenia, but only few studies have reported the relationship between P3 and AVH in schizophrenia (22).
Top-down inhibitory control measured in ERP often via the dichotic listening test, and the study have found that more dysfunctional top-down inhibition seemed to mediate the association between impairment to affective theory of mind and severity of hallucinations (23).
The Go/NoGo task is a classical paradigm, in which participants respond to the frequent “Go” stimuli as quickly as possible and avoid button pressing reaction in the infrequent “NoGo” stimuli (24, 25).
N2 and P3 in the Go/NoGo task are closely related inhibitory control (26–28). Despite intensive investigations, the AVH remains a poorly understood feature of schizophrenia. Many studies found that schizophrenia patients showed deficits in inhibitory control (29–31), but most of these studies did not make further analysis with regard to symptoms. Only a few studies argued that patients experiencing no AVH may not have obvious deficits in inhibitory control (18).
It is not clear whether the inhibitory control deficits in AVH patients stem from the disorder or the symptom. Additionally, results from Go/NoGo task may provide more support for inhibitory control deficits in AVH patients. Thus, in the present study, we aim to investigate inhibitory top-down control in schizophrenia patients with and without AVH using a Go/NoGo task.
reference link :https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8211872/
More information: Rick A. Adams et al, Computational modelling of EEG and fMRI paradigms indicates a consistent loss of pyramidal cell synaptic gain in schizophrenia, Biological Psychiatry (2021). DOI: 10.1016/j.biopsych.2021.07.024



{kind=link}