










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



But other than making people feel good, do these “mechanotherapies” actually improve healing after severe injury?
According to a new study from researchers at Harvard’s Wyss Institute for Biologically Inspired Engineering and John A. Paulson School of Engineering and Applied Sciences (SEAS), the answer is “yes.”
This process also removed inflammatory cytokines released by neutrophils from the muscles, enhancing the process of muscle fiber regeneration. The research is published in Science Translational Medicine.
“Lots of people have been trying to study the beneficial effects of massage and other mechanotherapies on the body, but up to this point it hadn’t been done in a systematic, reproducible way. Our work shows a very clear connection between mechanical stimulation and immune function.
This has promise for regenerating a wide variety of tissues including bone, tendon, hair, and skin, and can also be used in patients with diseases that prevent the use of drug-based interventions,” said first author Bo Ri Seo, Ph.D., who is a Postdoctoral Fellow in the lab of Core Faculty member Dave Mooney, Ph.D. at the Wyss Institute and SEAS.
A more meticulous massage gun
Seo and her coauthors started exploring the effects of mechanotherapy on injured tissues in mice several years ago, and found that it doubled the rate of muscle regeneration and reduced tissue scarring over the course of two weeks. Excited by the idea that mechanical stimulation alone can foster regeneration and enhance muscle function, the team decided to probe more deeply into exactly how that process worked in the body, and to figure out what parameters would maximize healing.
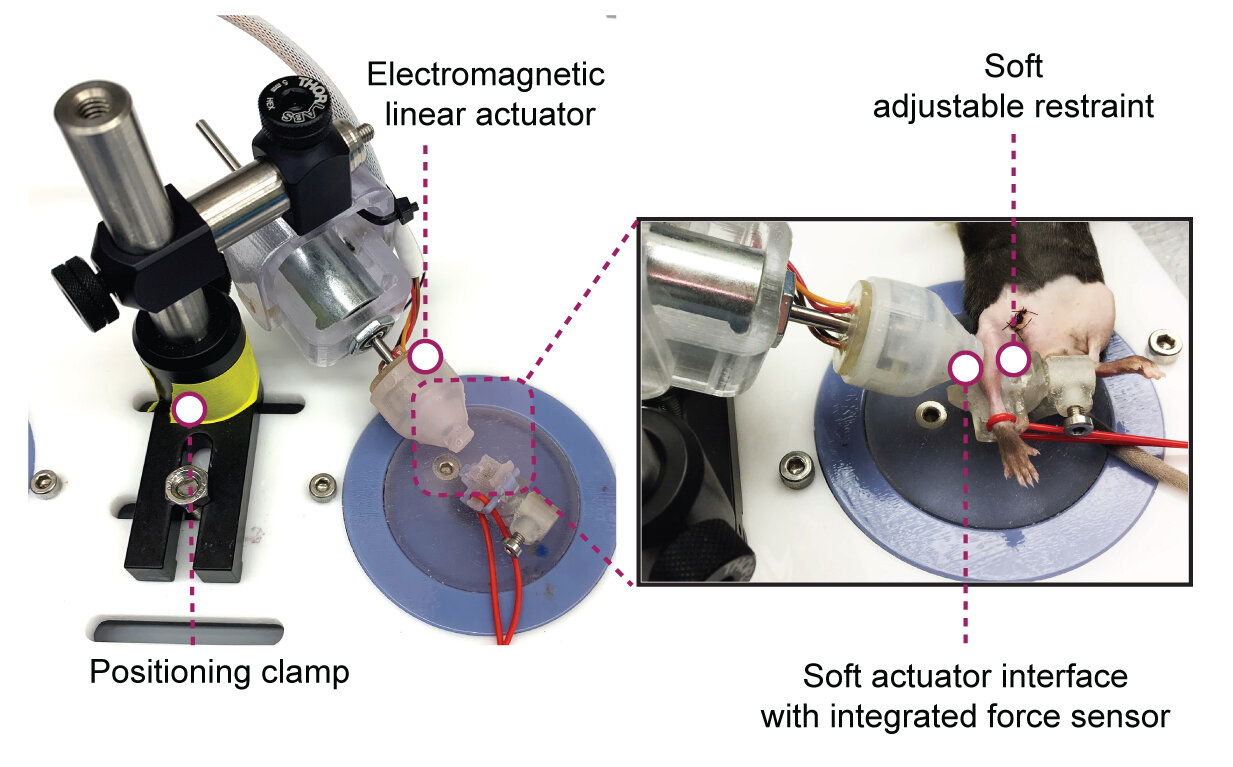
They teamed up with soft robotics experts in the Harvard Biodesign Lab, led by Wyss Associate Faculty member Conor Walsh, Ph.D., to create a small device that used sensors and actuators to monitor and control the force applied to the limb of a mouse.
The device we created allows us to precisely control parameters like the amount and frequency of force applied, enabling a much more systematic approach to understanding tissue healing than would be possible with a manual approach,” said co-second author Christopher Payne, Ph.D., a former Postdoctoral Fellow at the Wyss Institute and the Harvard Biodesign Lab who is now a Robotics Engineer at Viam, Inc.
Once the device was ready, the team experimented with applying force to mice’s leg muscles via a soft silicone tip and used ultrasound to get a look at what happened to the tissue in response. They observed that the muscles experienced a strain of between 10-40%, confirming that the tissues were experiencing mechanical force.
They also used those ultrasound imaging data to develop and validate a computational model that could predict the amount of tissue strain under different loading forces.
They then applied consistent, repeated force to injured muscles for 14 days. While both treated and untreated muscles displayed a reduction in the amount of damaged muscle fibers, the reduction was more pronounced and the cross-sectional area of the fibers was larger in the treated muscle, indicating that treatment had led to greater repair and strength recovery.
The greater the force applied during treatment, the stronger the injured muscles became, confirming that mechanotherapy improves muscle recovery after injury. But how?
Evicting neutrophils to enhance regeneration
To answer that question, the scientists performed a detailed biological assessment, analyzing a wide range of inflammation-related factors called cytokines and chemokines in untreated vs. treated muscles. A subset of cytokines was dramatically lower in treated muscles after three days of mechanotherapy, and these cytokines are associated with the movement of immune cells called neutrophils, which play many roles in the inflammation process.
Treated muscles also had fewer neutrophils in their tissue than untreated muscles, suggesting that the reduction in cytokines that attract them had caused the decrease in neutrophil infiltration.
The team had a hunch that the force applied to the muscle by the mechanotherapy effectively squeezed the neutrophils and cytokines out of the injured tissue. They confirmed this theory by injecting fluorescent molecules into the muscles and observing that the movement of the molecules was more significant with force application, supporting the idea that it helped to flush out the muscle tissue.
To pick apart what effect the neutrophils and their associated cytokines have on regenerating muscle fibers, the scientists performed in vitro studies in which they grew muscle progenitor cells (MPCs) in a medium in which neutrophils had previously been grown.
They found that the number of MPCs increased, but the rate at which they differentiated (developed into other cell types) decreased, suggesting that neutrophil-secreted factors stimulate the growth of muscle cells, but the prolonged presence of those factors impairs the production of new muscle fibers.
“Neutrophils are known to kill and clear out pathogens and damaged tissue, but in this study we identified their direct impacts on muscle progenitor cell behaviors,” said co-second author Stephanie McNamara, a former Post-Graduate Fellow at the Wyss Institute who is now an M.D.-Ph.D. student at Harvard Medical School (HMS).
“While the inflammatory response is important for regeneration in the initial stages of healing, it is equally important that inflammation is quickly resolved to enable the regenerative processes to run its full course.”
Seo and her colleagues then turned back to their in vivo model and analyzed the types of muscle fibers in the treated vs. untreated mice 14 days after injury. They found that type IIX fibers were prevalent in healthy muscle and treated muscle, but untreated injured muscle contained smaller numbers of type IIX fibers and increased numbers of type IIA fibers. This difference explained the enlarged fiber size and greater force production of treated muscles, as IIX fibers produce more force than IIA fibers.
Finally, the team homed in on the optimal amount of time for neutrophil presence in injured muscle by depleting neutrophils in the mice on the third day after injury. The treated mice’s muscles showed larger fiber size and greater strength recovery than those in untreated mice, confirming that while neutrophils are necessary in the earliest stages of injury recovery, getting them out of the injury site early leads to improved muscle regeneration.
“These findings are remarkable because they indicate that we can influence the function of the body’s immune system in a drug-free, non-invasive way,” said Walsh, who is also the Paul A. Maeder Professor of Engineering and Applied Science at SEAS and whose group is experienced in developing wearable technology for diagnosing and treating disease. “This provides great motivation for the development of external, mechanical interventions to help accelerate and improve muscle and tissue healing that have the potential to be rapidly translated to the clinic.”
The team is continuing to investigate this line of research with multiple projects in the lab. They plan to validate this mechanotherpeutic approach in larger animals, with the goal of being able to test its efficacy on humans. They also hope to test it on different types of injuries, age-related muscle loss, and muscle performance enhancement.
“The fields of mechanotherapy and immunotherapy rarely interact with each other, but this work is a testament to how crucial it is to consider both physical and biological elements when studying and working to improve human health,” said Mooney, who is the corresponding author of the paper and the Robert P. Pinkas Family Professor of Bioengineering at SEAS.
“The idea that mechanics influence cell and tissue function was ridiculed until the last few decades, and while scientists have made great strides in establishing acceptance of this fact, we still know very little about how that process actually works at the organ level.
This research has revealed a previously unknown type of interplay between mechanobiology and immunology that is critical for muscle tissue healing, in addition to describing a new form of mechanotherapy that potentially could be as potent as chemical or gene therapies, but much simpler and less invasive,” said Wyss Founding Director Don Ingber, M.D., Ph.D., who is also the Judah Folkman Professor of Vascular Biology at (HMS) and the Vascular Biology Program at Boston Children’s Hospital, as well as Professor of Bioengineering at SEAS.
ACUTE RESPONSE OF NEUTROPHILS TO EXERCISE
If inflammation is regarded as the proliferation of WBCs after soft tissue injury, then the cellular inflammatory response actually begins at the onset of exercise, when the circulating level of neutrophils increases significantly. 5–8 Neutrophils are the first WBC population to arrive and affect the host inflammatory response during exercise and soft tissue injury ( Table).
These cells have both specific and nonspecific defensive mechanisms, some of which are capable of causing additional tissue damage. 15–18 In the past, the early effects of damaging eccentric exercise were proposed to result in increased numbers of circulating neutrophils, as these cells would be required to enter the injury site to initiate phagocytosis or removal of damaged tissues.
However, this immediate response has also been observed after both noninjurious passive stretching and isometric exercise, illustrating that the presence of neutrophils does not necessarily always lead to injury. 19

The mechanism for early neutrophilia postexercise is likely due to a combination of factors. During rest, more than half of the circulating neutrophils are marginated along the endothelial walls of blood vessels. At the onset of exercise, increases in epinephrine, blood flow, and cell-signaling molecules demarginate these neutrophils away from the vessel walls, resulting in their mobilization into the circulation. 5, 20, 21 Demargination allows the neutrophils to enter the circulation and redistribute elsewhere in the body, as needed. The mechanisms by which neutrophils localize in damaged or stressed tissue are just beginning to be understood and may represent key strategies for intervention to limit certain aspects of inflammation.
The movement of a neutrophil from the circulation into the tissue, called diapedesis, is under tight regulatory control of the underlying tissue. In skeletal muscle, diapedesis can occur rapidly during exercise. 22 Neutrophil recruitment is ultimately the responsibility of the muscle fibers (myocytes) together with mast cells from a variety of tissues, including the local connective tissue. If a myocyte is perturbed in some fashion, such as in the case of an active stretch or contusion, it communicates with the endothelial wall of the adjacent blood vessel, initiating a cascade of signaling events and resulting in diapedesis. This intercellular communication is accomplished, in part, by a series of cell-signaling molecules, or cytokines, that are essential to any understanding of immune cell function.
The term cytokine is derived from the Greek root meaning “to put cells into motion.” 17 All nucleated cells in the body produce cytokines and similarly express cytokine receptors on their surface membranes. Cytokines act at the surface of the target cells, principally to alter cell function. 23
Skeletal muscle continually produces cytokines in an effort to maintain homeostasis and to regulate function. Simple perturbations of skeletal muscle, such as an active stretch during eccentric exercise, markedly increase the expression of interleukin-1β (IL-1β) and tumor necrosis factor–α (TNF-α). 24
These proinflammatory cytokines upregulate the expression of endothelial-leukocyte adhesion molecules (E-selectin) within the endothelium of the adjacent blood vessels. 17, 25, 26 Activation of the endothelium is site specific and can result in the release of additional IL-1β, as well as additional proinflammatory cytokines, including IL-6 and IL-8, both of which have been shown to attract neutrophils. 27–31
Thus, endothelial activation serves 2 purposes: encouraging the adhesion of neutrophils at the site of cell stress (margination) and assisting the cell in recruiting additional neutrophils ( Figure 1).

Modified muscle use may result in an increased intracellular calcium concentration, resulting in an increased cell production of proinflammatory cytokines such as TNF-α and IL-1β, which in turn upregulate the expression of endothelial-leukocyte adhesion molecules (E-selectin and P-selectin). The activated endothelium attracts neutrophils to the region and also releases the neutrophil chemoattractants and proinflammatory cytokines IL-6 and IL-8. IL-6 indicates interleukin 6; IL-8, interleukin 8; IL-1β, interleukin 1-beta; TNF-α, tumor necrosis factor–alpha; 1β; TNF-α, tumor necrosis factor–α; and ECM, extracellular matrix.
The temporary adhesion of neutrophils to the endothelium results in their immobilization and, hence, prolonged signaling from the muscle cell. 32 Without margination, no effective communication would be possible between the myocytes and the neutrophils, because these cell types would not be in close proximity for an adequate length of time.
This cytokine-mediated communication results in a reorganization of neutrophil 33, 34 and endothelial 35, 36 cell structure, allowing the neutrophils to pass from the endothelium (diapedesis) to the extracellular matrix (ECM) adjacent to the myocytes.
The traditional thinking has been that these cytokines were released only by injured or damaged myocytes, resulting in the localization of neutrophils to these injured tissues. This finding has been observed after eccentric contractions 4, 37 and has led to speculation that inflammation is the process responsible for delayed-onset muscle soreness. 19, 20, 38
However, simple muscle activation and passive stretch have recently been shown to be sufficient stimuli for diapedesis to occur, with subsequent localization of neutrophils within the ECM of skeletal muscle. 39, 40 Currently, researchers are focused on the mechanisms for neutrophil recruitment and the function of these neutrophils in otherwise healthy, uninjured muscle.
Among the most important questions regarding neutrophils and inflammation is whether the localization of neutrophils in the ECM facilitates healing or tissue destruction. Evidence is beginning to indicate that it is more likely a combination of both repair and further damage. The latter seems somewhat surprising but may even be an important signal for tissue repair.
CLINICAL IMPLICATIONS
Historically, the acute management of athletic musculoskeletal injury has focused on limiting the cardinal signs of inflammation in an effort to expedite the rehabilitative process and to facilitate an early return to competition. 81 To this end, the use of ice, compression, and elevation for initial management of injuries has flourished.
Over the last 25 years, rationales for acute treatment practices have changed, focusing on retarding secondary injury in an effort to minimize total injury. 82, 83 Regardless of the rationale, the practice of using ice, compression, and elevation in managing acute inflammation is well ingrained. Although a potential role for the use of physical agents, such as cryotherapy, in attenuating the neutrophilic response has been demonstrated in the laboratory, 84, 85 the actual clinical evidence supporting the efficacy of these practices is limited.
Similarly, limiting inflammation and enhancing tissue repair through the suppression of neutrophil recruitment and activation may reduce tissue damage postexercise. Such efforts have been established, as nonsteroidal inflammatory drugs (NSAIDs) have been used for centuries in an attempt to limit the inflammatory response. However, the anti-inflammatory effects may be confounded by the analgesic action of these drugs, 86 which has long been the focus of early interventions for muscle injury. 81
It has been suggested that the magnitude of pain after tissue trauma corresponds to the concentration of WBCs within the injured tissue. 87 However, this theory has not been supported in the literature. For example, although tendinitis is a common diagnosis, the absence of WBCs in tissues affected by this condition indicates that this is not a true inflammatory response. 88
Conversely, the mere presence of WBCs does not always coincide with the cardinal signs of inflammation. White blood cells have been observed in the absence of obvious tissue trauma, 39 even though this situation is generally not referred to as an inflammatory process.
A challenge to reducing inflammation through pharmacologic intervention is the multiple cellular pathways by which the inflammatory response can be mediated. Traditional NSAIDs block the cyclooxygenase (COX) pathway that contributes to cell-mediated prostaglandin (PGE 2) production 89 and, arguably, neutrophil recruitment. 90 However, other proinflammatory pathways exist for the cell to recruit neutrophils to damaged or exercised muscle, including the alternative lipoxygenase pathway 91 and the nuclear factor kappa-B (NF-κB)–mediated induction of proinflammatory genes. 92
Although a great deal of information on the efficacy of NSAID use exists in the literature, the immediate and long-term use of NSAIDs to control inflammation remains controversial. This may be due to the multiple proinflammatory pathways, the wide variety of emerging NSAIDs designed to target specific cellular pathways, and their respective effects of muscle repair and regeneration.
The effects of NSAIDs on inflammatory cell accumulation in the muscle and their relationship with muscle repair remain controversial. 44 For instance, inhibition of NF-κB by curcumin has been shown to accelerate muscle regeneration. 93 Although non–NF-κB inhibitors such as the NSAID naproxen have been shown to have no effect on muscle cell regeneration, 94 NS-398 (a COX-2–specific inhibitor) reduced neutrophil and macrophage entry into the muscle, delayed regeneration and healing, and resulted in increased TGF-β1 and increased tissue fibrosis. 89
Evidence is accumulating that NSAIDs may actually interfere with satellite cell proliferation, differentiation, and fusion 89, 95 and, therefore, may adversely affect muscle regeneration and repair. 89, 96, 97 Similarly, inhibited tissue repair after NSAID administration has also been shown after injury in other soft tissues, including ligaments. 98 Ultimately, although NSAID treatment for soft tissue injuries is common in sports medicine settings, no concrete evidence demonstrates that such treatments are justified, even for the analgesic effects. 99
If it is beneficial to limit the neutrophilic response, then the timing and dosage of NSAIDs are likely important. Neutrophils are the dominant immune cells for the first 4 to 24 hours postinjury, after which macrophages predominate. 3 Some potential clearly exists for limiting the neutrophil-mediated damage that appears to accompany mechanical stress to muscle and other tissues.
However, whether more is to be gained by combating the secondary neutrophilic damage but potentially interfering with the muscle regeneration process or by accepting the secondary damage in hopes that faster regeneration is stimulated remains unclear. It is important to note that evidence of impeding regeneration 75 was observed in neutrophil-depleted mice. That is, regeneration was impaired in an animal model in which no neutrophils were present, indicating that neutrophils may play a key role in muscle repair.
Although this laboratory model is useful, it does not reflect the clinical reality of acute intervention in the injured athlete. Completely abolishing the neutrophilic response using typical clinical cryotherapy or NSAID therapy would be practically impossible. Therefore, we expect that some level of neutrophilic response would be seen, regardless of our acute intervention. No data presently describe whether a partially muted response would be beneficial or harmful.
In skeletal muscle, the propensity for an enhanced inflammatory response and fibroblast proliferation exceeds the muscle’s ability to regenerate, particularly in humans, resulting in the formation of a fibrotic scar. Until recently, this fibrotic response was presumed to be a necessary step in the formation of nascent myotubes for muscle fiber repair.
However, fibrotic scar formation is not an optimal outcome and may be due to excessive cell signaling 100 and inflammatory response. 101 When the function of fibroblasts and TGF-β1 was inhibited after laceration injuries, skeletal muscle had the inherent ability to regenerate damaged fibers. 102–104 Although this finding has not been studied in models of severe strain injury, the manipulation of cell signaling may provide a glimpse into the possible future of therapeutic agents designed to modify tissue healing.
Clinically, return to activity can result in an exacerbation of the inflammatory response. 105 However, evidence is also accumulating that regular exercise acts as an anti-inflammatory agent. 106 Neutrophil function and cytotoxicity may be modified through exercise, 107 and these modifications may depend on exercise intensity. 21 The production of cytokines by neutrophils as well as the resulting response from all WBCs can be modified with long-term exercise. 15
The exact mechanisms are not known, but the low-level inflammatory response produced through regular exercise may blunt the cells’ response to cytokines or inhibit their production and subsequent release. In this regard, regular exercise may suppress the release of proinflammatory cytokines, such as TNF-α. 106 Recently, using isolated chondrocytes, the proinflammatory response was shown to vary depending on the magnitude of the mechanical signal applied to the tissue. 108 Thus, exercise may produce both proinflammatory and anti-inflammatory effects, depending on the magnitude of the stimulus and the corresponding level of cytokine released.
reference link:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1748424/
More information: Skeletal muscle regeneration with robotic actuation–mediated clearance of neutrophils, Science Translational Medicine (2021). www.science.org/doi/10.1126/scitranslmed.abe8868



{kind=link}