









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



In their paper, they note that very little is currently known about why some individuals are immune to COVID-19, but they suggest that a stronger effort to find out could lead to new ways to treat or prevent the disease.
The authors note that the pandemic has served to remind the global community of the remarkable variability in viral response—some people are asymptomatic while others get so sick that they die.
They note also the clear differences that researchers have observed; for instance, cases in which a single person in a family remains uninfected while everyone around them gets sick; or people who work in a high-risk environment but who do not get sick.
The authors also note that as of right now, no one really knows why there is such variability in response to SARS-CoV-2 infections, though there are clues. There have been some reports that people with type O blood, for example, suffer less when infected.
And there have been other studies that suggest certain proteins produced by the body are more or less active when confronted with the SARS-CoV-2 virus. It has also been revealed that the virus needs proteins that have receptors such as ACE2 or TMEM41B. If people lack the receptors, the virus is unable to replicate.
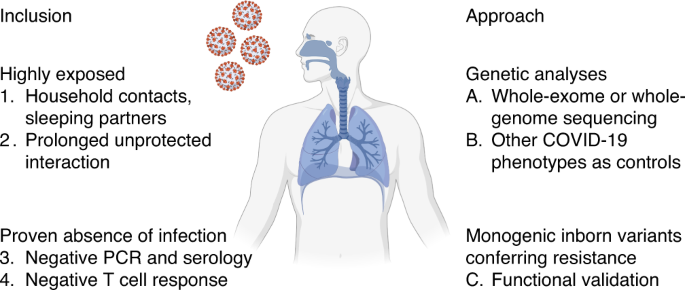
Such a study would involve subjects who believe they should have been infected with the disease. Most particularly, such an effort would need to actively recruit members of a household where one person remains uninfected.
They also state that the initial steps of such a study are already underway – 400 volunteers meeting the required criteria have already signed on.
The authors conclude by noting that the nature of the pandemic has suggested that the SARS-CoV-2 virus is not going away anytime soon; thus, it would be beneficial if the science community could fully understand why people respond so differently when exposed to it.
In this longitudinal cohort study, the presence of anti-spike antibodies was associated with a substantially reduced risk of PCR-confirmed SARS-CoV-2 infection over 31 weeks of follow-up. No symptomatic infections and only two PCR-positive results in asymptomatic health care workers were seen in those with anti-spike antibodies, which suggests that previous infection resulting in antibodies to SARS-CoV-2 is associated with protection from reinfection for most people for at least 6 months. Evidence of postinfection immunity was also seen when anti-nucleocapsid IgG or the combination of anti-nucleocapsid and anti-spike IgG was used as a marker of previous infection.
The incidence of SARS-CoV-2 infection was inversely associated with baseline anti-spike and anti-nucleocapsid antibody titers, including titers below the positive threshold for both assays, such that workers with high “negative” titers were relatively protected from infection. In addition to the 24 seronegative health care workers with a previous positive PCR test, it is likely that other health care workers with baseline titers below assay thresholds, which were set to ensure high specificity,23 had been previously infected with SARS-CoV-2 and had low peak postinfection titers or rising or waning responses at testing.5
Two of the three seropositive health care workers who had subsequent PCR-positive tests had discordant baseline antibody results, a finding that highlights the imperfect nature of antibody assays as markers of previous infection. Neither worker had a PCR-confirmed primary SARS-CoV-2 infection. Subsequent symptomatic infection developed in one worker, and both workers had subsequent dual antibody seroconversion. It is plausible that one or both had false positive baseline antibody results (e.g., from immunoassay interference27). The health care worker in whom both anti-spike and anti-nucleocapsid antibodies were detected had previously had PCR-confirmed SARS-CoV-2 infection; the subsequent PCR-positive result with a low viral load was not confirmed on repeat testing and was not associated with a change in IgG response. These results could be consistent with a reexposure to SARS-CoV-2 that did not lead to symptoms but could also plausibly have arisen from undetected laboratory error; although contemporaneous retesting of the PCR-positive sample was not undertaken, samples tested 2 and 4 days later were both negative. If the PCR-positive result is incorrect, the incidence rate ratio for PCR positivity if anti-spike IgG–seropositive would fall to 0.05. We detected and did not include in our analysis a presumed false positive PCR test in a fourth seropositive health care worker.
Owing to the low number of reinfections in seropositive health care workers, we cannot say whether past seroconversion or current antibody levels determine protection from infection or define which characteristics are associated with reinfection. Similarly, we cannot say whether protection is conferred through the antibodies we measured or through T-cell immunity, which we did not assess. It was not possible to use sequencing to compare primary and subsequent infections, since only one of the three seropositive health care workers with a subsequent PCR-positive test had PCR-confirmed primary infection and that worker’s original sample was not stored. Our study was relatively short, with up to 31 weeks of follow-up. Ongoing follow-up is needed in this and other cohorts, including the use of markers of both humoral and cellular immunity to SARS-CoV-2, to assess the magnitude and duration of protection from reinfection, symptomatic disease, and hospitalization or death and the effect of protection on transmission.
Health care workers were enrolled in a voluntary testing program with a flexible follow-up schedule, which led to different attendance frequencies. Although health care workers were offered asymptomatic PCR testing every 2 weeks, the workers attended less frequently than that (mean, once every 10 to 13 weeks). Therefore, asymptomatic infection is likely to have been underascertained. In addition, as staff were told their antibody results, “outcome ascertainment bias” occurred, with seropositive staff attending asymptomatic screening less frequently. However, a sensitivity analysis suggests that the differing attendance rates did not substantially alter our findings. Staff were told to follow guidance on social distancing and use of personal protective equipment and to attend testing if Covid-19 symptoms developed, even if the worker had been previously PCR- or antibody-positive. This is reflected in the similar rates of testing of symptomatic seropositive and seronegative health care workers.
Some health care workers were lost to follow-up after terminating employment at our hospitals; this was likely to have occurred at similar rates in seropositive and seronegative staff. Not all PCR-positive results from government symptomatic testing sites were communicated to the hospital. This is a study of predominantly healthy adult health care workers 65 years of age or younger; further studies are needed to assess postinfection immunity in other populations, including children, older adults, and persons with coexisting conditions, including immunosuppression.
In this study, we found a substantially lower risk of reinfection with SARS-CoV-2 in the short term among health care workers with anti-spike antibodies and those with anti-nucleocapsid antibodies than among those who were seronegative.
reference link :https://www.nejm.org/doi/full/10.1056/NEJMoa2034545
Historical examples of inborn resistance to infection with other pathogens provide a road map for testing the hypothesis of monogenic inborn resistance to infection with SARS-CoV-2. Some more common inborn variants of resistance in candidate genes may have relatively small effects. However, we also aim to identify candidate genes with potentially rare variants and a large effect size. These variants are of particular interest for two reasons.
First, they can provide a deep understanding of the essential biological pathways involved in infection with SARS-CoV-2. Second, they will allow for the development of innovative therapeutic interventions to prevent or treat SARS-CoV-2 infection in others.
The proof-of-principle for this second reason of interest has been provided by CCR5 and its antagonist maraviroc, which is used for the treatment of HIV-1 infections in specific settings79. In addition, transplantation of CCR5-deficient bone marrow has been successfully applied to cure HIV infection in a few people80,81.
No specific drug effective against COVID-19 has been discovered since the start of the pandemic. Lessons learned from experiments of nature could potentially guide us toward such specific treatments for COVID-19. We have already enrolled more than 400 individuals meeting the criteria for inclusion in a dedicated resistance study cohort.
The collaborative enrollment of study participants is continuing (http://www.covidhge.com), and subjects from all over the world are welcome.
More information: Evangelos Andreakos, A global effort to dissect the human genetic basis of resistance to SARS-CoV-2 infection, Nature Immunology (2021). DOI: 10.1038/s41590-021-01030-z



{kind=link}