










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



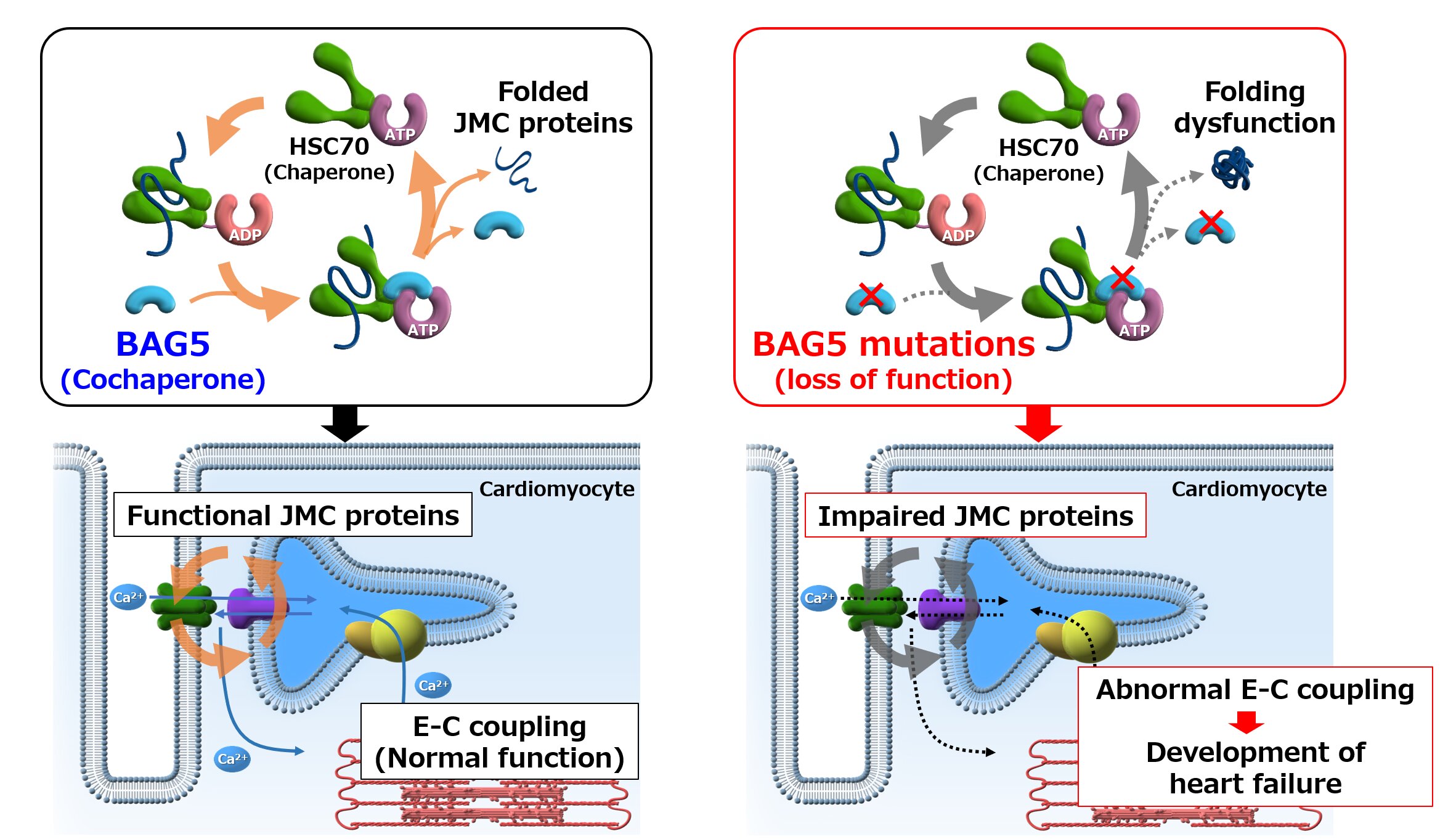
This gene, BAC5, is important for the movement of calcium ions in the heart muscle and calcium ions are what drives the pumping of the heart.
The good news is that the investigators also found a way to fix the mutation through a novel gene therapy approach, demonstrating a potential treatment for this devastating disease.
In a study published this month in the journal Science Translational Medicine, researchers from Osaka University have shown that a previously unknown mutation can lead to a condition called dilated cardiomyopathy, which is one of the main causes of heart failure.
Heart failure is an incurable condition where the heart is no longer able to meet the body’s demands in terms of blood supply. It is one of the most common causes of death and it affects almost 40 million people worldwide, representing a huge public health problem. One of the main factors leading to heart failure is a disease called dilated cardiomyopathy (or DCM).
DCM is characterized by dilation of the heart’s chambers and a pumping disfunction. Previous research has shown that DCM is often inherited and has a genetic basis. However, for up to 80% of the familial DCM cases, we still don’t know the genetic mutation causing the disease.
They then found in a mouse model of dilated cardiomyopathy that mice without BAG5 exhibited the same symptoms of human DCM, such as dilatation of the heart’s chambers and irregular heart rhythm. This indicates that mutations that erase the function of BAG5 can cause cardiomyopathy.
“Here we showed that loss of BAG5 perturbs calcium handling in mouse cardiomyocytes,” says Dr. Hideyuki Hakui, lead author of the study. BAG5 is important for calcium handling in the heart muscle cells, and calcium is essential for a regular rhythm and overall health of the cardiac muscle, explaining why a loss of BAG5 leads to cardiomyopathy.
“After demonstrating that BAG5 mutations led to loss of functional BAG5 protein,” continues Dr. Yoshihiro Asano, senior author of the study, “we also showed that administration of an AAV9-BAG5 vector in a murine model could restore cardiac function. This finding suggests that gene therapy with adeno-associated viruses (AAV) should be further investigated as a possible treatment alternative to heart transplantation for patients who are BAG5 deficient.”
Diabetes is a major health problem worldwide, responsible for approximately 5 million deaths in 2017, with an increasing incidence expected to reach 693 million by the year 2045 [1]. One of the leading causes of death (approximately 50%) in people with diabetes is cardiovascular disease. In particular, the prevalence of heart failure in diabetic patients is reportedly increased by 6–8-fold in the 45- to 65-year-old age-group compared with non-diabetic individuals [2].
Moreover, diabetes alone can accelerate the development of heart failure in individuals with pre-existing cardiac pathologies (such as myocardial infarction), resulting in poorer prognosis compared with non-diabetic individuals [3]. The accompanying abnormalities in cardiac structure and function are collectively termed ‘diabetic cardiomyopathy’ or diabetes-associated heart failure, originally defined as cardiomyopathy not directly attributable to hypertension or coronary disease.
This phenomenon has been known for at least 5-decades [4–7]; however, diabetic cardiomyopathy still remains the subject of intense research to understand the key causal signalling pathways to target for future therapeutic development.
AAV-based therapeutics represent a new frontier in clinical medicine
Treatment options for cardiovascular diseases have advanced significantly in recent years, as a result of improved understanding of the molecular pathways involved in cardiac damage [39,40]. In particular, the use of gene therapy has proven to be one of the most promising avenues to treat various types of diseases, including heart failure [40]. Aimed at the correction of key pathologies, gene therapy involves the delivery of therapeutic genes of interest to a specific tissue target.
Successful incorporation of the delivered gene allows the endogenous cell machinery to produce the specific encoded protein [41,42]. The success of gene therapy depends heavily on the efficient transfer of the genetic material to the tissue of interest, which is facilitated by different delivery strategies. Early delivery methods included the use of naked plasmid DNA, liposomal DNA complexes, polymer-carrying DNA and oligonucleotides [43].
Delivery of naked plasmids to tissues, however, does not provide sufficient transfection into the tissue of interest [44,45]. Furthermore, rapid systemic degradation of plasmids and poor cellular entry are other limitations [40,46,47]. In contrast, non-pathogenic viral approaches have been shown to be a more superior method as the vector for gene delivery [45,46]. Notably, AAVs have been demonstrated to exhibit the best risk-benefit profile and will be the focus for the remainder of this review.
Brief introduction to AAV principles
Derived from the Parvoviridae family, AAVs are non-enveloped single-stranded DNA vectors, with a favourable safety profile and the capability of achieving persistent transgene expression in a wide range of target tissues, including cardiac tissue [48]. AAVs are relatively small (20 nm) and therefore limited in their packaging capacity of only around 4.7 kb [47]. Yet one of the most attractive features of AAV vectors is the continued expression of the transgene for a prolonged period of time [40,49], despite the extrachromosomal location of the vector [47].
However, the infrequent integration of the vector means that transduction must occur in cells that either do not replicate or do so very slowly [47]. Cardiomyocytes are an excellent example of cells that are considered the most compatible for use of AAV gene therapy, as cardiomyocyte turnover is negligible in adults [50]. For in vivo gene delivery, recombinant AAVs (rAAV) are commonly used, which have the same sequence and structure as a wild-type AAV, but are devoid of all AAV-protein coding sequences [51].
AAVs enter the cell via glycosylated cell surface receptors, triggering clathrin-mediated endocytosis (Figure 2) [51]. Utilising the cytoskeletal network AAVs advance through the cytosol, undergoing conformational modification in response to a change in pH [51]. AAVs are then released by the endosome, where they enter the nucleus and release their content.
The viral inverted terminal repeats (ITRs) present in the rAAV genome can drive inter- or intra-molecular recombination to form circularised episomal genomes that can persist in the nucleus. Vector genomes can also undergo integration into the host genome at very low frequencies; however, this is a very rare occurrence unlike both lentiviral and retroviral that can randomly integrate into the host genome to disrupt normal gene function [52]. Moreover, compared with adenoviruses which were a popular vector choice in the early 2000s, AAVs has been shown to be excellent to evade the innate immune system [53] and considered highly safe and potent compared with other vectors.

Principles of AAV-mediated gene therapy
Adeno-associated virus (AAV) binds to the host glycosylated cell surface receptor to trigger clathrin-mediated endocytosis internalization. The AAV then moves through the cytosol via the cytoskeletal network. Conformational changes are then triggered by pH changes in the cellular environment, leading to endosomal release. The AAV undergoes transport to the nucleus, releasing its cargo, where it is then transcribed into double-stranded DNA for transcription, or undergoes integration to the host genome (which rarely occurs). Messenger RNA produced from transcription of the cargo leads to its translation to the protein-of-interest outside of the nucleus. Production of this protein-of-interest then enables the cardioprotective effects that are observed in response to AAV-mediated gene therapy.
reference link:https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8187922/
More information: “Loss-of-function mutations in the co-chaperone protein BAG5 cause dilated cardiomyopathy requiring heart transplantation,” Science Translational Medicine (2022). DOI: 10.1126/scitranslmed.abf3274



{kind=link}