









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



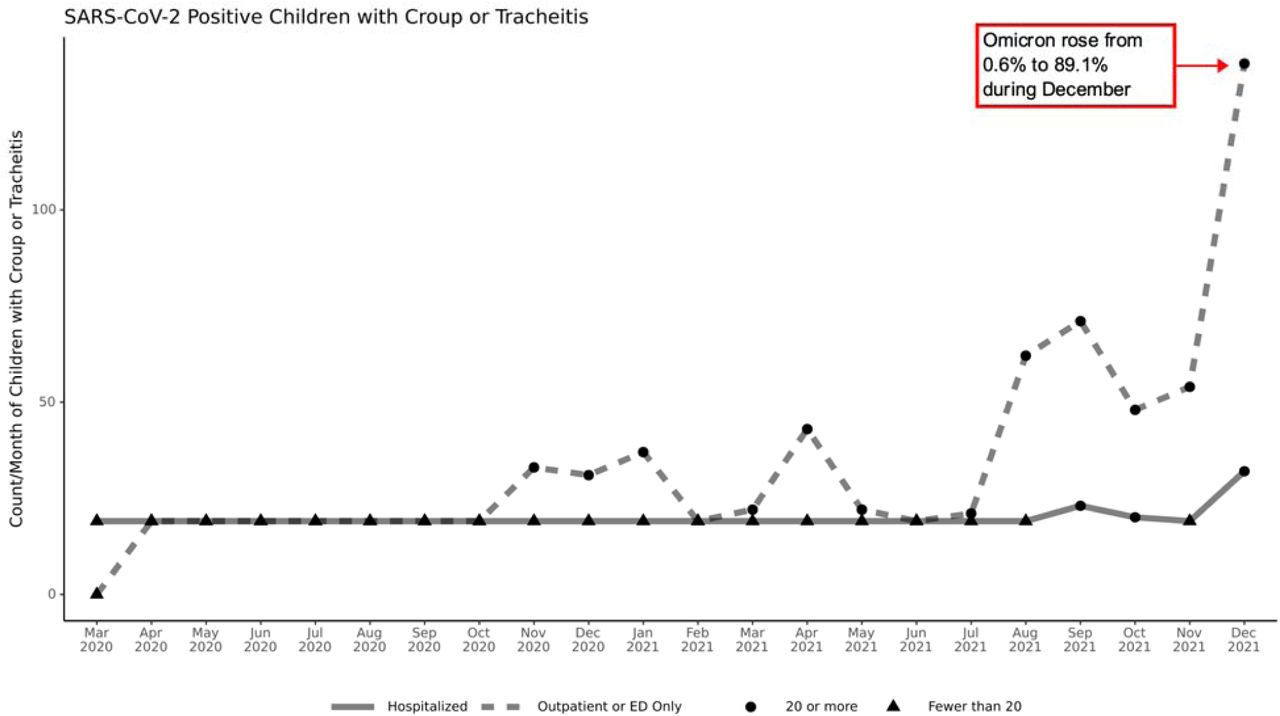
Researchers from University of Colorado School of Medicine-USA, Northwestern University Feinberg School of Medicine-USA and Stony Brook University-USA have in a new retrospective cohort study discovered that pediatric acute upper airway infection cases have increased exponentially during Omicron variant surge in the United States.
Physicians elsewhere around the globe that are experiencing the Omicron surge are also reporting of the same occurrences among children and it is important that both parents and teachers are aware of this.
Numerous reports of SARS-CoV-2 causing laryngotracheobronchitis (commonly known as croup) have been limited to small number of documented case series.
Preliminary published reports suggest the Omicron (B.1.1.529) strain of SARS-CoV-2 (the dominant circulating US strain since the week of 12/25/2021) replicates more efficiently in the conducting airways. This may increase the risk of a croup phenotype in children as they have smaller airway calibers.
The study findings were published on a preprint server and are currently being peer reviewed. https://www.medrxiv.org/content/10.1101/2022.01.27.22269865v1
Results
Overall, the 1/13/2022 N3C data release contains 15,806 hospitalized SARS-CoV-2 positive children, of whom 1.5% (234/15,806) had UAI (Table 1). Compared to those without UAI, those with UAI were more likely to be male (59.8% versus 50.4%, p=0.003), younger (2.4 versus 10.1 years, p<0.001), white (54.7% versus 43.3%, p=0.02), and have asthma (15% versus 10%, p=0.02). Children with UAI experienced severe disease (invasive ventilation, vasopressors, ECMO, or mortality) more often compared to children without UAI (31.6% versus 13.5%, p<0.001).

Discussion
Overall, pediatric acute UAI has increased during the Omicron variant surge. Nearly a third of affected children develop severe disease. This observed clinical phenotype of pediatric infection by the Omicron variant appears to confirm recent mechanistic reports.
A limitation of this analysis is that diagnosis codes will only be present for completed hospitalizations in N3C; children who are still hospitalized are not represented.
Although many children with acute UAI are managed as outpatients, those with severe croup and/or tracheitis are at risk of cardiac arrest from rapid-onset upper airway obstruction.
They may require therapies typically provided in intensive care units including frequent administration of nebulized racemic epinephrine, helium/oxygen mixtures, and intubation. While SARS-CoV-2 pediatric UAI rates are not overwhelmingly high, understanding this new clinical phenotype is important to health systems under severe strain.



{kind=link}
{kind=link}