










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



In their paper published in The Journal of Neuroscience, the group describes how they built on their prior research to learn more about the ways adolescents mature into independent people.
In 2016, the same team conducted a research effort that involved studying the brains of children as they responded to their mothers’ voices. They found that young children could not only accurately identify their mother’s voice, but that hearing it triggered a host of processing areas in the brain. In this new effort, the researchers expanded on these findings by conducting similar tests on the brains of children as they grew into adolescence.
The new work involved making audio recordings of volunteer mothers saying nonsense words. The researchers then played the recordings for the teenage offspring of the mothers during fMRI scans, which highlighted the parts of the brain that were activating. The researchers also played other random sounds and the voices of people that were not known to the volunteers.
Eventually, they responded more to unknown voices than to their mother’s voice. More specifically, they found that the voice-selective superior temporal sulcus became more active in the teens as they grew older when hearing almost any voice.
Adolescent Development
Adolescence is a period of significant development that begins with the onset of puberty1 and ends in the mid-20s. Consider how different a person is at the age of 12 from the person he or she is at age 24. The trajectory between those two ages involves a profound amount of change in all domains of development—biological, cognitive, psychosocial, and emotional. Personal relationships and settings also change during this period, as peers and romantic partners become more central and as the adolescent moves into and then beyond secondary school or gains employment.
Importantly, although the developmental plasticity that characterizes the period makes adolescents malleable, malleability is not synonymous with passivity. Indeed, adolescents are increasingly active agents in their own developmental process. Yet, as they explore, experiment, and learn, they still require scaffolding and support, including environments that bolster opportunities to thrive. A toxic environment makes healthy adolescent development challenging. Ultimately, the transformations in body, brain, and behavior that occur during adolescence interact with each other and with the environment to shape pathways to adulthood.
Each stage of life depends on what has come before it, and young people certainly do not enter adolescence with a “blank slate.” Rather, adolescent development is partly a consequence of earlier life experiences. However, these early life experiences are not determinative, and the adaptive plasticity of adolescence marks it as a window of opportunity for change through which mechanisms of resilience, recovery, and development are possible. (Chapter 3 discusses this life-course perspective on development in detail.) This chapter explores three key domains of adolescent development: puberty, neurobiological development, and psychosocial development. Within each domain, we highlight processes that reflect the capacity for adaptive plasticity during adolescence and beyond, marking adolescence as a period of unique opportunity for positive developmental trajectories.
PUBERTY
Puberty, a normative developmental transition that all youth experience, is shaped by both social and biological processes. Although often misconstrued as an abrupt, discrete event, puberty is actually a gradual process occurring between childhood and adolescence and one that takes many years to complete (Dorn and Biro, 2011). Biologically, puberty involves a series of complex alterations at both the neural and endocrine levels over an extended period that result in changes in body shape (morphology), including the maturation of primary and secondary sex characteristics during late childhood and early adolescence and, ultimately, the acquisition of reproductive maturity (Dorn and Biro, 2011; Natsuaki et al., 2014).
Two biological components of puberty, adrenarche and gonadarche, are relevant in understanding the link between puberty and adolescent wellbeing. Adrenarche, which typically begins between ages 6 and 9, refers to the maturation of the hypothalamic-pituitary-adrenal (HPA) axis, during which the levels of adrenal androgens (e.g., dehydroepiandrosterone and its sulfate) begin to increase. While adrenarche begins in late childhood, levels of adrenarchal hormones continue to rise throughout adolescence, peaking in the early 20’s (Blakemore et al., 2010). Adrenal androgens contribute to the growth of pubic and axillary hair. Gonadarche typically begins in early adolescence, at approximately ages 9 to 11, and involves the reactivation of the hypothalamic-pituitary-gonadal (HPG) axis (for a review, see Sisk and Foster, 2004).2 The rise of gonadal steroid hormones to adult levels occurs as a result of HPG reactivation and is primarily responsible for breast and genital development in girls.
The consequence of these complex changes in HPA and HPG axes at the neuroendocrine level is a coordinated series of visible, signature changes in body parts. These include a growth spurt, changes in skin (e.g., acne) and in body odor, the accumulation of body fat (in girls), the appearance of breast budding (in girls) and enlargement of testes and increased penis size (in boys), the growth of pubic and axillary hair, the growth of facial hair (in boys), and the arrival of the first period (i.e., menarche, in girls). Key pubertal events are highlighted in Figure 2-1; however, as discussed next, there is a great deal of variation in the timing and tempo of these events.
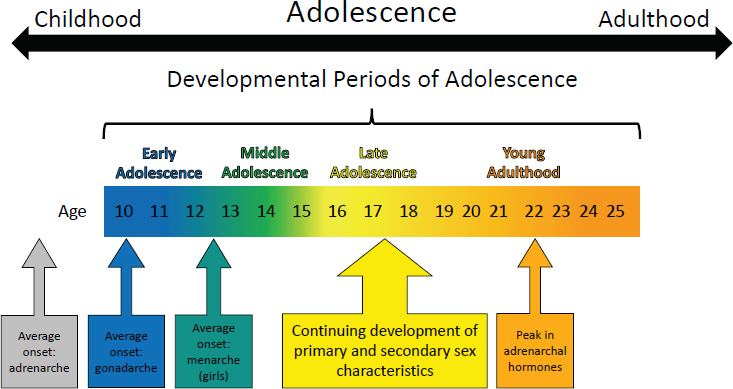
FIGURE 2-1. Key pubertal events across adolescence.
It is useful to distinguish three distinct yet interrelated ways to conceptualize individual differences in pubertal maturation. Pubertal status refers to how far along adolescents are in the continuum of pubertal maturation at any given moment. For instance, if an 11-year-old girl has just experienced menarche, she is considered to have advanced pubertal status because menarche is the last event that occurs in the process of the female pubertal transition. Pubertal status is inherently confounded with age, because older adolescents are more likely to have attained advanced pubertal status.
Pubertal timing, on the other hand, refers to how mature an adolescent is when compared to his or her same-sex peers who are of the same age. In other words, pubertal timing always includes a reference group of one’s peers. For example, a girl who experiences menarche at age 10 may be an earlier maturer in the United States, because her menarcheal timing is earlier than the national average age for menarche nationwide, which was found to be 12.4 years in a cohort of girls born between 1980 and 1984 (McDowell et al., 2007). Only 10 percent of girls in the United States are estimated to have experienced menarche before 11.11 years of age (Chumlea et al., 2003), suggesting that the girl in this example would be considered to have early pubertal timing. Unlike pubertal status, pubertal timing is not confounded by age because, by definition, pubertal timing is inherently standardized within same-sex, same-age peers typically residing in the same country.
Pubertal tempo is a within-the-individual metric that refers to how quickly a person completes these sets of pubertal changes. For example, some boys may experience a deepening of their voice and the development of facial, axillary, and pubic hair all within a matter of months, whereas other boys may have a gap of several years between voice-deepening and the development of facial hair. Pubertal tempo has gained more attention recently with the rise of sophisticated longitudinal methodology and the resulting availability of longitudinal data on pubertal maturation (e.g., Ge et al., 2003; Marceau et al., 2011; Mendle et al., 2010).
Regardless of the metric used, most of the research on adolescent pubertal development has focused on girls. We know comparatively little about the processes, correlates, and outcomes of pubertal maturation in boys, except for the well-replicated findings that girls typically begin and complete puberty before boys. Evidence is now emerging that the relationship between puberty and structural brain development in the amygdala and hippocampus region may differ by sex (Satterthwaite et al., 2014; Vijayakumar et al., 2018). These sex differences in associations between brain development and puberty are relevant for understanding psychiatric disorders characterized by both hippocampal dysfunction and prominent gender disparities during adolescence.
It is also important to consider the pubertal development of transgender and gender-nonconforming youth. Transgender and gender-nonconforming individuals usually identify as a gender other than the one they were assigned at birth (Sylvia Rivera Law Project, 2012). Individuals who are gender-nonconforming may identify as transgender, genderqueer, gender-fluid, gender-expansive, or nonbinary. Puberty is a time that can be enormously stressful, and the fear of developing—or the actual development of—secondary sexual characteristics that do not match a child’s gender identity can be intense and even destabilizing (de Vries et al., 2011). Some transgender and gender-nonconforming youth might take medications that block puberty. Although puberty blockers have the potential to ease the process of transitioning, the long-term health effects of these drugs are not yet known (Boskey, 2014; Kreukels and Cohen-Kettenis, 2011).
The Role of Early Experiences on Pubertal Timing and Tempo
As noted earlier, the timing and rate of pubertal development vary greatly. The age at which someone matures is due to a combination of genetic and environmental influences (e.g., Mustanski et al., 2004). Early life experiences, including social risks and disadvantages, have been shown to accelerate pubertal tempo and lower the age of pubertal timing (Marshall and Tanner, 1969). Specifically, accelerated pubertal tempo and early pubertal timing have been associated with stressors, including childhood sexual abuse and physical abuse, obesity, prematurity, light exposure, father absence, and exposure to endocrine disruptors (such as chemicals in plastics, pesticides, hair-care products, and many meat and dairy items) (see e.g., Steinberg, 2014, pp. 54–55). This section reviews the literature on associations between these early experiences and normative variations in pubertal timing and tempo. We close this section with a brief discussion of these associations as a marker of adaptive plasticity.
Maltreatment
One of the most widely studied early experiences related to pubertal development is child maltreatment, and in particular, sexual abuse. A series of studies shows that the age of menarche tends to be lower for girls who experienced child sexual abuse as compared to girls who have not experienced this (Bergevin et al., 2003; Natsuaki et al., 2011; Romans et al., 2003; Turner et al., 1999; Wise et al., 2009). Trickett and Putnam (1993) suggested that the trauma of child sexual abuse introduces physiological as well as psychological consequences for children, including accelerated maturation by premature activation of the HPA and HPG axes. In addition, some studies have observed a relationship between childhood physical abuse and early maturation, though less robustly and less consistently than for sexual abuse (Bergevin et al., 2003; Wise et al., 2009), and these studies do not always control for the possibility of concurrent sexual abuse (e.g., Romans et al., 2003).
In one of the few studies to examine pubertal development longitudinally in adolescents with maltreatment histories, Mendle and colleagues (2011) followed a sample of 100 girls in foster care at four points in time over 2 years, beginning in the spring of their final year of elementary school. The previously established association between sexual abuse and earlier onset of maturation and earlier age at menarche was replicated, and in addition, physical abuse was found to be related to a more rapid tempo of pubertal development. A recent longitudinal study of 84 sexually abused girls and matched-comparison girls replicated the association between sexual abuse and earlier pubertal onset (including breast development and pubic hair; Noll et al., 2017). Further, using this same sample, childhood sexual abuse predicted earlier pubertal development which, in turn, was associated with higher levels of internalizing symptoms such as depression and anxiety concurrently and 2 years later (Mendle et al., 2014). A third study with this sample found that earlier-maturing girls were more anxious in the pre- and peri-menarche periods than their later-maturing peers; however, their anxiety declined after menarche, suggesting a time-limited effect on mental health and the potential for recovery upon completion of pubertal maturation, as girls enter later adolescence (Natsuaki et al., 2011).
The association between sexual abuse and earlier pubertal development was recently replicated using a large population-based sample of adolescents, the National Longitudinal Study of Adolescent Health3 (N = 6,273 girls). In that study, child sexual abuse predicted earlier menarche and development of secondary sexual characteristics, whereas other types of maltreatment did not (Mendle et al., 2016). The distinctive role for early pubertal timing suggests that the heightened sexual circumstances of puberty may be especially challenging for girls whose lives have already been disrupted by adverse early experiences, yet also suggests a potential opportunity for intervention and resilience, particularly in later adolescence, once pubertal development is complete. However, the vast majority of research in this area has focused solely on girls, and we know very little about whether maltreatment is also associated with earlier pubertal timing in boys.
Other Family and Health Factors
Other family factors that may be stress-inducing yet much less extreme than maltreatment have also been associated with pubertal timing and tempo. For example, Quinlan (2003) found that the number of caretaking transitions a child experiences was associated with earlier menarche. Sung and colleagues (2016) found that exposure to greater parental harshness (but not unpredictability) during the first 5 years of life predicted earlier menarche; and a recent meta-analysis found that father absence was significantly related to earlier menarche (Webster et al., 2014), although genetic confounding may play a role in this association (Barbaro et al., 2017).
Health factors that may affect the metabolic system are also predictive of pubertal timing. For example, in girls, low birth weight (Belsky et al., 2007) and obesity/higher body mass index (BMI) (Wagner et al., 2015) have both been associated with earlier pubertal maturation. For boys, overweight (BMI ≥ 85th and < 95th percentile) has been associated with earlier pubertal maturation, whereas obesity (BMI ≥ 95th percentile) was associated with later pubertal maturation (Lee et al., 2016), suggesting a complex association between aspects of the metabolic system and puberty in boys.
Environmental Exposures
Recently, researchers have examined whether a child’s exposure to chemicals is related to pubertal maturation by serving as an endocrine disruptor (see e.g., Lomniczi et al., 2013; Simonneaux et al., 2013; Steingraber, 2007). In the first longitudinal study of age of pubertal timing and exposure to persistent organic pollutants—chemicals used in flame retardants—researchers found that the age at pubertal transition was consistently older in participants who were found to have higher chemical concentrations in collected blood samples (Windham et al., 2015). The effects of neuroendocrine disruptors on girls’ pubertal timing may begin during the prenatal period, as there is evidence that female reproductive development is affected by phthalate or bisphenol A exposure during specific critical periods of development in the mother’s uterus (Watkins et al., 2017).
Accelerated Maturation and Adaptive Plasticity
It is clear that early experiences can factor into accelerated pubertal timing and tempo, and theorists suggest that this may be adaptive. According to Mendle and colleagues (2011, p. 8), “age at certain stressful life transitions represents a dose-response relationship with maturation, with earlier ages at these events associated with earlier development (e.g., Ellis and Garber, 2000).” Belsky et al. (1991) posited that children who are raised in harsh, stressful environments may have accelerated pubertal development to compensate for a mistrust of commitment and of investment in social relationships. According to Belsky and colleagues, early pubertal timing may serve the evolutionary biological purpose of elongating the window for reproductivity and fertility, to permit more conceptions in a lifetime. Thus, the well-documented association between adverse early life experiences and early pubertal development may itself be an adaptive response, one that reflects the plasticity in neurobiological systems during adolescence to adapt to the specific socio-cultural context.
The Social Context of Pubertal Maturation
Despite the role that stressful early life events play in accelerating pubertal timing, it is important to note that adolescence is also a period of potential for recovery. Even when an adolescent has experienced early adversity and this has precipitated earlier pubertal maturation, the social context in which that adolescent is developing can ultimately change the trajectory of their outcomes—for better or worse. For example, closer and less conflict-laden parent-child relationships can reduce associations between pubertal maturation and behavior problems, while more conflict-laden and less close relationships exacerbate them (Booth et al., 2003; Dorn et al., 2009; Fang et al., 2009). Parental knowledge of an adolescent child’s whereabouts and activities also plays a role, as the influence of pubertal timing on problematic outcomes is weakened when such parental knowledge of adolescent whereabouts and activities is high, and it is amplified when knowledge is low (Marceau et al., 2015; Westling et al., 2008). During early childhood, a secure infant-mother attachment can buffer girls from the later effects of harsh environments on earlier pubertal maturation (Sung et al., 2016).
The Context of Biological Sex and Gender Norms
The biological changes of puberty take place in social and cultural contexts, and these dynamic person-context interactions have implications for adolescent development. For instance, the physical changes associated with pubertal maturation affect an adolescent’s self-image as much as the way he or she is treated and responded to by others (Graber et al., 2010), and culturally grounded gender norms may make these associations more salient for girls than boys. Indeed, in the United States, although menstruation is acknowledged as a normal biological event, it is nevertheless often accompanied by feelings of shame and the need to conceal it from others, particularly males (Stubbs, 2008). As a result, the arrival of a girl’s first menstrual cycle is often accompanied by embarrassment and ambivalence (Brooks-Gunn et al., 1994; Moore, 1995; Tang et al., 2003), as well as by negative feelings (Rembeck et al., 2006), including anxiety, surprise, dismay, panic, and confusion (Brooks-Gunn and Ruble, 1982; Ruble and Brooks-Gunn, 1982).
The arrival of puberty has other social consequences, such as changing dynamics and maturing relationships with parents, siblings, and peers, as well as the emergence of peer relationships with adults. Pubertal maturation is associated with a higher incidence of sexual harassment, both by peers of the same gender and across genders (McMasters et al., 2002; Petersen and Hyde, 2009; Stattin and Magnusson, 1990). Social consequences may be exacerbated among youth experiencing early pubertal timing.
The increase in pubertal hormones (e.g., estradiol, progesterone, testosterone, dehydroepiandrosterone) and the changes they drive, such as the emergence of secondary sex characteristics, is also associated with the development of substance use (Auchus and Rainey, 2004; Grumbach, 2002; Grumbach and Styne, 2003; Havelock et al., 2004; Matchock et al., 2007; Oberfield et al., 1990; Terasawa and Fernandez, 2001; Young and Altemus, 2004). At the same time, the causal direction of these findings is somewhat mixed (Castellanos-Ryan et al., 2013; Dawes et al., 1999; Marceau et al., 2015), with variation by sex. In girls, relatively early pubertal timing and faster pubertal tempo often mark an increased risk for adolescent substance use (Cance et al., 2013; Castellanos-Ryan et al., 2013; Costello et al., 2007; Lee et al., 2014). By contrast, in boys later pubertal timing and/or slower pubertal tempo mark an increased risk for substance use (Davis et al., 2015; Marceau et al., 2015; Mendle and Ferrero, 2012). This striking gender difference in associations between pubertal maturation and substance use highlights how the same biological event (pubertal maturation) can lead to very different outcomes as a function of one’s biological sex.
Puberty and Stress Sensitivity
Puberty-related hormones influence the way adolescents adjust to their environment, for example by experiencing symptoms of depression and anxiety. One mechanism through which this might occur is in pubertal hormones’ ability to alter sensitivity to stress, making adolescent girls particularly sensitive to exogenous stressors. Recent studies using salivary cortisol as an index of stress regulation have documented heightened stress reactivity and delayed post-stress recovery in pubescent adolescents (Gunnar, et al., 2009; Stroud et al., 2004; Walker et al., 2004). Cortisol is a steroid hormone released by the HPA axis, and disruption to this axis has been implicated in the development of symptoms of depression and anxiety (e.g., Gold and Chrousos, 2002; Guerry and Hastings, 2011; Sapolsky, 2000).
In fact, cortisol secretion is closely intertwined with age, puberty, and sex, which together appear to contribute to adolescent girls’ vulnerability to external stressors (Walker et al., 2004; Young and Altemus, 2004). As will be discussed in Chapter 3, cortisol, along with neuroendocrine, autonomic, immune, and metabolic mediators, usually promotes positive adaptation in the body and the brain, such as efficient operation of the stress response system. However, when cortisol is over- or under-produced it can, along with the other mediators, produce negative effects on the body and brain, such as forming insulin resistance and remodeling the brain circuits that alter mood and behavior. At the same time, as will be shown in Chapter 3, interventions during adolescence have the potential to mediate the harmful effects of stress.
reference link :https://www.ncbi.nlm.nih.gov/books/NBK545476/
More information: Daniel A. Abrams et al, A neurodevelopmental shift in reward circuitry from mother’s to nonfamilial voices in adolescence, The Journal of Neuroscience (2022). DOI: 10.1523/JNEUROSCI.2018-21.2022



{kind=link}