










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Associate Professor Kelvin Tan from UQ’s Business School says the statistic is a key finding of a study into the impacts different country characteristics, such as leadership, have had on COVID-19 infection and death rates.
“Countries where women were at the head of government outperformed countries with male leadership, with an average 39.9% fewer confirmed COVID-19 deaths,” Dr. Tan said.
“This figure can be attributed to female leaders taking quick and decisive action, a broader view of the wider impact on society and being more receptive to innovative thinking.
“We found female leaders tend to act promptly and decisively and are more risk-averse towards the loss of human life, which play an essential role in pandemic prevention and outcomes,” he said.
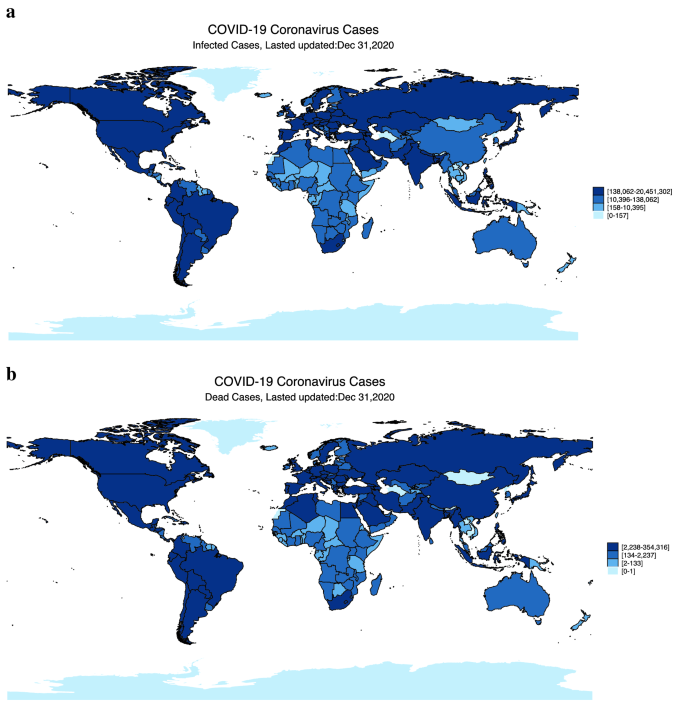
Dr. Tan said many countries adopted similar approaches to contain the spread of COVID-19, but there were drastic differences in morbidity and mortality, even among those with similar socio-economic conditions and political backgrounds like Australia and New Zealand.
“As of 31 December 2020, although the population of Australia was only five times that of NZ, Australia had reported around 13 times more infections and 36 times the number of deaths than the numbers reported by New Zealand,” he said.
The study found gender ratio, population density, urbanization and political corruption all intensified the severity of a country’s pandemic experience.
“We’ve identified a set of predetermined, country-specific characteristics that have significantly influenced the outcomes of the pandemic and we hope policymakers use them to manage risk during future health emergencies,” Dr. Tan said.
“Our findings highlight the importance of prevention, rather than treatment, in reducing COVID-19 morbidity and mortality.”
The research is published in Scientific Reports.
Our analysis of the relation between 21 predetermined, country-specific factors and COVID-19 outcomes suggests that multiple factors are required to explain country-level performances in the battle against COVID-19. Ex-post contingent interventions are certainly crucial; however, pre-existing country characteristics exogenous to the outbreak can explain a substantial part of pandemic outcomes.
To mitigate pandemic severity and risk, populous countries should remain on alert because most work and social activities occurs domestically, and population acts as a decisive aggravating factor for pandemic outbreaks. Since most countries are moving toward an aging population, it is crucial to protect the elderly, who are especially vulnerable during pandemics. As a result of urbanization, higher population density is unavoidable in many economies. Therefore, governments should strive to achieve a balance between the efficient utilization of urban spaces and sufficient social spaces for disease prevention in the layout design of housing and communities.
Both authoritarian and democratic governments must act in a unified and timely manner to manage health crises. For democratic countries, democracy itself is not to blame; rather, it is about whether leaders can strike a delicate balance between authority and liberal rights during the crisis. Policies should be put in place to allow governments to make centralized decisions in a health crisis, as delays in interventions can result in life and death consequences.
In an outbreak, the life of every person is linked to the choices and behaviors of others; first and foremost, everyone has the right to secure their health. Thus, we believe that it is right and just for governments to develop awareness among the citizenry about the importance of sacrifices (e.g., loss of mobility) during critical periods of pandemic outbreaks. Governments and citizens should act in unity and prioritize pandemic control, even at the expense of reducing a certain degree of freedom in both political and individual domains. Factors (e.g., corruption) that give rise to inefficiencies in government, which, in turn, destroy trust in government, must be eradicated. Our findings suggest that democracy must be accompanied by a strong government for successful pandemic control. As Henderson55 observes, “as the pandemic has made clear, strong government—democratically accountable government, balanced by a free media and a thriving private sector—is the price we pay for strong societies”.
The fact that COVID-19 has affected some developed countries more than developing countries indicates that economic power does not imply immunity to a health crisis. It is not the financial resources of a country but the timeliness and effectiveness of interventions that primarily determine the success of pandemic controls. Countries would be wise to realize that it is not only GDP that matters but also how such resources are allocated, and the endeavor to invest more resources in public health and disease prevention in addition to advances in medicine.
Income inequality within a country can cause health disparities, and governments should consider health as a public good, making preventive healthcare as widely accessible as possible. Our findings on the heightening effect of income inequality on COVID-19 severity suggest that public policies should direct special attention to protecting the poor, who are more vulnerable to pandemics. Countries that rely heavily on tourism inflows may need to prepare for increased health risks associated with the spread of infectious diseases, in addition to those risks related to the inevitable reductions in income resulting from the effects of the pandemic on travel.
To enhance the mitigating factors, investment in education has proved fruitful, even leading to an improvement in public health. Education enables citizens to make more informed health-related decisions. The control of a pandemic requires the participation and cooperation of every individual as citizens join governments to co-create social values. Countries should continue to develop the knowledge of citizens, especially as technologies (e.g., contact tracing) become instrumental for crisis management. Technological innovation can facilitate infectious disease control and ensure that infected people are identified, traced, and treated in a timely manner, all of which can alleviate severe consequences in pandemics.
It is unrealistic to expect all countries to choose female leaders. However, perhaps male leaders could learn from their female counterparts and pay more attention to issues that matter to the health of the broader population and society. Trust in government, law, and order, which take a long time to develop, build a country’s resilience and have proved instrumental during both peace and crises. Past experience of similar health crises helps governments and citizens stay alert and better prepared for new health crises, as seen in countries with a history of SARS or similar. Investment in healthcare facilities pays off when a crisis escalates, but is justifiable with or without a crisis.
To conclude, we identify a set of predetermined country characteristics that significantly influence the outcomes of COVID-19. Country-specific factors can either strengthen or attenuate a country’s resilience to the pandemic. Our results have implications for policymakers, healthcare experts, and the public. Policymakers and healthcare experts may consider utilizing these factors to further develop risk-preparedness and strengthen social solidarity in health crises.
Despite its contributions, this study has at least two major limitations. The first relates to its reliance on reported infection cases and deaths. Reported figures may vary significantly across countries in terms of timeliness, accuracy, completeness, and consistency. For example, Belgium, a developed country, has aggressively reported COVID deaths that occurred in elderly-care homes based on symptoms and contacts, even without confirmed diagnosis. In contrast, some developing or authoritarian countries may have severely underreported the number of fatalities. Further, in countries with limited testing capacities, only the most seriously ill people can be tested.
As such, many infected individuals who were asymptomatic may not have been included in our dataset. Such inequality in data quality and potential underreporting issues are a challenging—but potentially fruitful—avenue for future studies. Second, our study mainly focuses on the cross-sectional differences in COVID-19 outcomes at a given point in time. Thus, our analysis cannot reveal how and whether certain factors influence the transmission dynamics across countries, which would require time series models to explore the lead–lag relation among countries in confirmed cases and deaths. We leave this important issue for future research.
More information: Dianna Chang et al, The determinants of COVID-19 morbidity and mortality across countries, Scientific Reports (2022). DOI: 10.1038/s41598-022-09783-9



{kind=link}