











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A new study by German researchers from University Hospital Münster has alarmingly found that that SARS-CoV-2 virus leaves a persistent capillary rarefication (a reduction in vascular density) even 18 months after infection.
The study findings were published in the peer reviewed journal: Angiogenesis. (By Springer) https://link.springer.com/article/10.1007/s10456-022-09850-9
The long COVID cohort encompasses 27 adult patients, studied after a median (IQR) duration of 541 (305–569) days post-COVID-19 infection. The patients (55.5% men), aged 53 (39–51) years and had a median Charlson Comorbidity Index (CCI) of 0 (Table 1).
Table 1 Baseline characteristics
From: Persistent capillary rarefication in long COVID syndrome
| Variable | Healthy controls | Historical ICU COVID-19 cohort | Long COVID cohort | p value# | p value++ |
|---|---|---|---|---|---|
| Number of participants (n; %) | 15 | 16 | 27 | – | – |
| Female sex (n; %) | 8 (53.3) | 3 (13) | 12 (44.4) | 0.75 | 0.03 |
| Age [years, median (IQR)] | 53 (39–69) | 62 (56–72) | 53 (39–51) | 0.45 | 0.004 |
| BMI [kg/m2, median (IQR)] | 23.7 (22.0–25.2) | 27.3 (23.5–31.5) | 27.1 (23.2–29.1) | 0.17 | 0.74 |
| Hospitalized (n; %) | – | 16 (100) | 15 (55.5) | – | – |
| SOFA score [pts, median (IQR)] | – | 6 (2–13) | – | – | – |
| Vasopressors (n; %) | – | 6 (37.5) | – | – | – |
| Invasive mechanical ventilation (n; %) | – | 14 (87.5) | – | – | – |
| In-hospital mortality (n; %) | – | 6 (26.1) | – | – | – |
| Days after COVID-19 infection | – | 7 (1–17) | 541 (305–569) | – | < 0.001 |
| CCI score [median (IQR)] | 0 | 1 (0–3) | 0 (0) | 0.99 | 0.005 |
| Comorbidities (n; %) | |||||
| Arterial hypertension | 0 | 11 (68.8) | 4 (14.8) | 0.28 | < 0.001 |
| Diabetes mellitus | 0 | 0 | 0 | – | – |
| Chronic respiratory disease | 0 | 3 (18.8) | 2 (7.4) | 0.53 | 0.34 |
| Congestive heart failure | 0 | 6 (37.5) | 0 | 0.99 | 0.001 |
| Rheumatologic disease | 0 | 3 (17.2) | 3 (11.1) | 0.54 | 0.65 |
| Malignancy | 0 | 3 (18.8) | 1 (3.7) | 0.99 | 0.14 |
| Long COVID symptoms (n; %) | |||||
| > 1 Symptoms | – | – | 23 (85.2) | – | – |
| Fatigue/Weakness | – | – | 23 (85.2) | – | – |
| Dyspnea | – | – | 22 (81.5) | – | – |
| Chest discomfort | – | – | 6 (22.2) | – | – |
| Neurocognitive dysfunction | – | – | 4 (14.8) | – | – |
| Persistent cough | – | – | 2 (7.4) | – | – |
| Headache | – | – | 2 (7.4) | – | – |
| Sublingual videomicroscopy [median (IQR)] | |||||
| PBR (µm) | 2.23 (2.02–2.31) | 2.39 (2.13–2.52) | 2.15 (2.03–2.27) | 0.45 | 0.02 |
| Capillary density (10−2 mm/mm2) | 77.89 (66.66–83.27) | 19.88 (12.13–42.08) | 46.43 (39.15–63.49) | < 0.001 | < 0.001 |
| VRBC4–7 µm (µm/sec) | 103 (89.87–112.6) | 82.67 (75.03–95.53) | 114.9 (102.7–134.4) | 0.01 | < 0.001 |
| VRBC≥10 µm (µm/sec) | 100.60 (93.95–110.10) | 85.14 (97.12–69.55) | 124 (119.60–132.20) | < 0.001 | < 0.001 |
| MVHS (points) | 3.87 (3.15–4.87) | 0.92 (0.766–1.85) | 2.72 (2.21–3.01) | 0.002 | < 0.001 |
| Capillary recruitment (%)* | 70 | 17 | 29 | – | – |
- Bold indicates the statistically significant p values (p < 0.05)
- BMI Body mass index, CBV capillary blood volume, CCI score Charlson Comorbidity Index, COVID-19 Coronavirus disease 2019, CRP C-reactive protein, D capillary diameter, IQR interquartile range, MVHS Microvascular Health Score, PBR Perfused boundary region, PCT Procalcitonin, SOFA score Sequential Organ Failure Assessment score, VRBC red blood cell velocity
- *Capillary recruitment was estimated using 1 − slope (VRBC (D ≤ 7 µm), VRBC (D ≥ 10 µm)) in a per group analysis
- #p values were calculated between healthy controls and long COVID patients
- ++p values were calculated between historical COVID-19 cohort and long COVID patients
Long COVID patients showed a significantly lower vascular density compared to healthy controls. Specifically, a µm-precise analysis showed the decrease in vascular density to exclusively affect very small capillaries (D5: − 45.16%; D6: − 35.60%; D7: − 22.79%) (Fig. 1A). Compared with healthy controls, the capillary density of long COVID patients was decreased by 41% (Fig. 1B). However, glycocalyx dimensions did not differ from those of the healthy volunteers (Fig. 1C), even in a µm-precise analysis (data not shown). Upon recombination of these indices into MVHS™, severe impairment of the microcirculation in individuals with long COVID [healthy 3.87 (3.15–4.87) vs. long COVID 2.72 (2.21–3.01) points, p = 0.002; Fig. 1D] is emphasized. In a pooled analysis of the measurements of all study participants (n = 58), disease group (healthy controls, long COVID, historical acute COVID-19 cohort) was the only variable associated with the MVHS™. This association remained significant after adjustment for age, sex, CCI and BMI (β = − 0.52, p < 0.001).
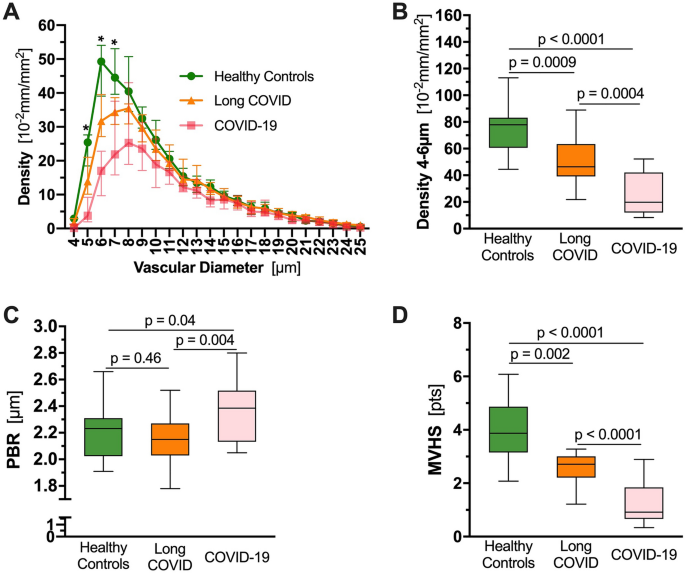
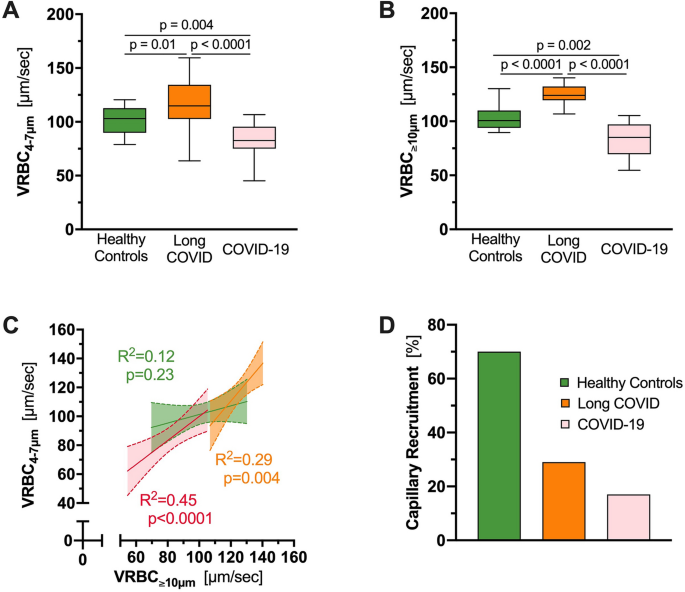
We previously used a ratio derived from VRBC in feed vessels relative to capillaries (VRBC (D ≥ 10 µm)/VRBC (D ≤ 7 µm) to calculate capillary recruitment (see above) [8]. Analysis of RBC velocity (VRBC) revealed significant differences between all three study groups, both in VRBC4–7 µm (Fig. 2A) and in VRBC≥10 µm (Fig. 2B). Surprisingly, VRBC was significantly higher in capillaries as well as feed vessels in long COVID patients compared with healthy individuals (VRBC4–7 µm: 114.9 [102.7–134.4] vs. 103 [89.87–112.6] µm/s, p = 0.01; VRBC≥10 µm: 124 [119.6–132.2] vs. 100.6 [93.95–110.1] µm/s; p < 0.0001). Plotting VRBC≥10 µm vs. VRBC4–7 µm revealed a strong dependency between capillaries and feed vessels in both, individuals with long COVID and hospitalized COVID-19 patients (long COVID: R2 = 0.29, p = 0.004; COVID-19: R2 = 0.45, p < 0.0001), indicating impaired capillary (de-)recruitment in these groups. In contrast, capillary VRBC was constant in healthy controls, indicating functioning (de-)recruitment of CBV associated with changes of feed vessel blood flow in healthy subjects (R2 = 0.12; p = 0.23) (Fig. 2C). CR was 29% in long COVID, 17% in COVID-19 patients and 70% in healthy volunteers (Fig. 2D). This finding suggests that the number of perfused capillaries in long COVID remains fixed and does not adequately respond to local variations of tissue metabolic demand. Associating the different symptoms with the capillary density in an explorative manner, revealed a statistically significant capillary rarefication in long COVID individuals presenting with neurocognitive dysfunction (38.50 [25.93–44.41] vs. 49.77 [43.40–64.30], p = 0.049; Supp. Table 1).
By further analyses, long COVID individuals showed no significant difference in MVHS or capillary density irrespective of outpatient or inpatient care—regardless of need for oxygen supplementation, during acute COVID-19 infection (Fig. 3A, C; Table 2). To assess recovery of microcirculatory parameters over time, we plotted MVHS and capillary density against the length of time between initial infection and presentation to the long COVID study outpatient clinic. Interestingly, no improvement of these parameters was documented, assuming capillary loss due to COVID-19 might be irreversible (Fig. 3B, D).
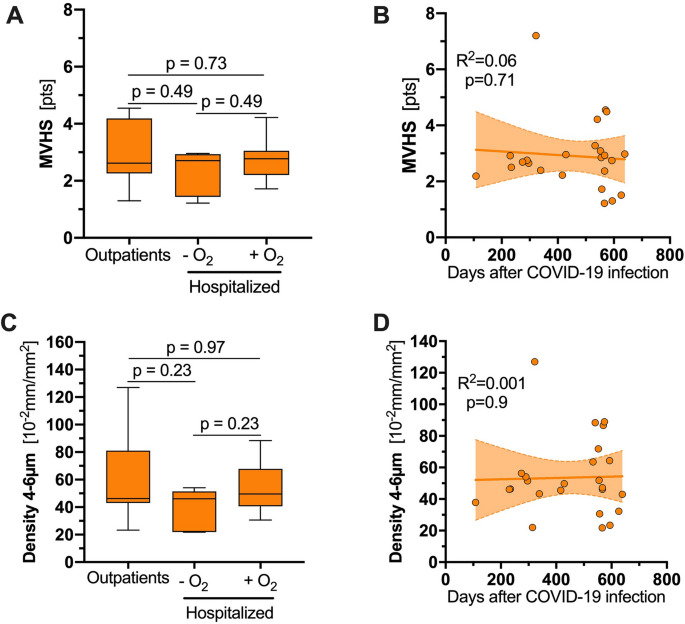
Table 2 Long COVID cohort divided with regard to the acute infection
From: Persistent capillary rarefication in long COVID syndrome
| Variable | Outpatient | Hospitalized without oxygen supplementation | Hospitalized with oxygen supplementation | p value* |
|---|---|---|---|---|
| Number of participants (n; %) | 12 | 7 | 8 | – |
| Female sex (n; %) | 8 (66.7) | 2 (28.6) | 2 (25) | 0.11 |
| Age [years, median (IQR)] | 54 (36–58) | 44 (32–63) | 59 (47–61) | 0.35 |
| BMI [kg/m2, median (IQR)] | 26.3 (21.2–29.1) | 26.6 (24–28) | 28.04 (24.72–29.30) | 0.67 |
| Critical illness (n; %) | – | – | 3 (37.5) | – |
| Days after COVID-19 infection | 550 (236–588) | 314 (290–566) | 553 (474–559) | 0.50 |
| CCI score [median (IQR)] | 0 (0–1) | 0 (0) | 0 (0) | 0.16 |
| Long COVID symptoms (n; %) | ||||
| > 1 Symptoms | 12 (100) | 5 (71.4) | 6 (75) | 0.15 |
| Fatigue/Weakness | 10 (83.3) | 7 (100) | 6 (75) | 0.39 |
| Dyspnea | 12 (100) | 5 (71.4) | 5 (62.5) | 0.08 |
| Chest discomfort | 4 (33.3) | 2 (28.6) | 0 (0) | 0.19 |
| Neurocognitive dysfunction | 1 (8.3) | 2 (28.6) | 1 (12.5) | 0.48 |
| Persistent cough | 2 (16.7) | 0 (0) | 0 (0) | 0.26 |
| Headache | 1 (8.3) | 0 (0) | 1 (12.5) | 0.65 |
| Sublingual videomicroscopy [median (IQR)] | ||||
| PBR (µm) | 2.15 (1.97–2.29) | 2.12 (2.03–2.31) | 2.16 (2.0–2.22) | 0.98 |
| Capillary density (10−2 mm/mm2) | 46.30 (43.03–81.04) | 46.16 (21.96–51.48) | 49.55 (40.64–67.92) | 0.36 |
| VRBC4–7 µm (µm/sec) | 119.84 (106.85–131.87) | 105.40 (94.89–126.47) | 121.99 (103.88–151.22) | 0.43 |
| VRBC≥10 µm (µm/sec) | 129.82 (120–130.72) | 123.24 (113.01–133.71) | 122.86 (119.09–131.96) | 0.87 |
| MVHS (points) | 2.62 (2.26–4.19) | 2.70 (1.44–2.93) | 2.77 (2.21–3.05) | 0.67 |
- *p values were calculated with the use of Kruskal–Wallis test among the three groups
Discussion
To the best of our knowledge, the present in vivo study is the first to address the microvasculature of long COVID individuals in a detailed, diameter class-wise manner. The number of small capillaries, but not of the supply vessels, were markedly reduced, very similar to the pattern found during severe COVID-19 infection [4].
In addition, capillary recruitment of COVID long-term patients remains significantly reduced. While healthy controls succeed in maintaining a constant capillary VRBC (almost horizontal slope), long COVID patients as well as acute COVID-19 patients fail to do so (steeper slopes). This finding reflects a persistent fixed number of perfused capillaries, which is insensitive to local tissue variations of metabolic demand [8].
To what extent this capillary rarefication is mechanical or/and functional remains unclear. Pretorius et al. revealed common clotting pathologies in plasma of acute and long COVID patients, further supporting the existence of persistent microthrombi [10]. Besides that, an insufficient recovery of the initial inflammation accompanied by persistent immunological abnormalities might also be responsible for the observed capillary impairment [6].
Previous studies focusing on the pulmonary [11], exertional [12] and myocardial [13] microcirculation of long COVID individuals showed local impairment of the microcirculation.
Our data complement these findings and point to a systemic and long-lasting capillary rarefication. This finding could possibly explain the functional impairment observed in long COVID syndrome. A subtle but exciting feature of the long-haul COVID group is, that the RBC velocities are the highest in our long COVID cohort (indicated by parallel shift of the slope to the upper right).
We speculate that this finding could represent a compensatory mechanism to meet metabolic demands. Considering that the measurements were taken at physical rest, it is quite conceivable that this presumed compensatory mechanism is exhausted more quickly during exertion than in healthy individuals, possibly explaining long COVID symptoms.
Here, we previously were able to present data on persistent exertional impairment caused by (micro-) circulatory reduction of the oxygen pulse during sequential, bicycle cardiopulmonary exercise test [12].
In the TUN-EndCOV Study, Charfeddine et al. reported a significant microvascular and endothelial dysfunction in a post-COVID cohort, evaluated by finger thermal monitoring after occlusion and reperfusion of the hand [14]. Specifically, long COVID individuals showed a higher endothelial quality index and a slower response to the reperfusion phase.
This finding was partially reversed after oral intake of sulodexide, a highly purified mixture of glycosaminoglycans, that includes fast-moving heparin and dermatan sulfate [15]. Indeed, our data imply that long COVID individuals respond inadequately to local variations of tissue metabolic demand.
Therefore, it is intriguing to speculate, that this delayed response after reperfusion might be the functional result of the observed capillary rarefication and the impaired capillary recruitment of the remaining capillaries in the long COVID individuals.
Regarding endothelial glycocalyx, previous studies have shown a trend towards partial recovery of the glycocalyx in the first months following the acute infection [16, 17]. Ikonomidis et al. evaluated PBR values of post-COVID individuals 12 months after infection, showing persistent glycocalyx impairment [18].
Here we demonstrate completely restored glycocalyx dimensions in long COVID individuals about 1.5 years after the acute infection. Mechanistically, glycocalyx thinning is tightly controlled, among others by the endothelium specific Angiopoietin(Angpt)/Tie2 system. We have shown that Angpt-2 activates heparanase release from the endothelium which leads to enzymatic degradation of the endothelial glycocalyx [19].
Indeed, we and others showed that both heparanase and Angpt-2 levels are elevated during the acute infection [4, 20]. Recent studies in long COVID reported normalized heparanase and Angpt-2 levels [21], consistent with restored glycocalyx dimensions. In this regard, our data once again highlight differential regulation of microcirculation parameters and glycocalyx dimensions, a finding we first observed in critically ill patients with bacterial sepsis [22].
We acknowledge some limitations. First, our pilot study had a small sample size and is mostly hypothesis-generating. Our study is observational and does not demonstrate causality between microvascular damage and post-COVID symptoms. Second, we included a historical cohort to better understand the microvascular changes.
However, all microvascular parameters were assessed under the same conditions using the same GlycoCheck camera by the same experienced investigator. Third, plasma samples are not available in our long COVID patients, so we cannot perform further analyses of endothelial markers. Fourth, the capillary recruitment was calculated post-hoc in a per group analysis; meanwhile a per individual analysis has become available which might provide even more accurate results.



{kind=link}