










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The study findings were published in the peer reviewed journal: Immunology.
https://onlinelibrary.wiley.com/doi/10.1111/imm.13577
Since 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to the recognition of the emergence of broad-spectrum multi-organ disease with increasing prevalence of cardiac injury in hospitalized patients. SARS-CoV-2 has been associated with a wide range of cardiac complications.
Specifically, the initial infection stage has been associated with acute myocardial injury [1-3] with abnormal echocardiography findings in both left and right ventricles [4], arrhythmias [1, 2], palpitations [5], myocarditis [6], heart failure [7] and other de novo problems [8, 9]. Paralleling these clinical symptoms is a growing body of evidence of increased cardiac complications in patients who have recovered from COVID-19 [10].
Ongoing myocardial inflammation and LGE [15] have also been reported even in patients who recovered from relatively mild, or even asymptomatic, COVID-19. Individuals who have recovered from mild COVID-19 suffer an increased burden of arrhythmias, chest pain, heart failure and vascular complications compared to uninfected patients, and this sequelae has been accompanied by excess use of drug therapies [16]. Currently, it remains unclear how long-term cardiac complications from COVID-19 will persist in convalescent patients. Studies have shown that the risk and 1-year burden of cardiovascular disease is substantial in survivors of acute COVID-19 [17].
Virus-induced cardiac complications are not unique to SARS-CoV-2 infection. Influenza A virus (IAV) infection has been frequently associated with myocardial injury and infarction, endocarditis, tachycardia, ST segment echocardial changes and atrial fibrillation [18, 19], mostly resolving within a year of infection [19].
Evidence of SARS-CoV-2 direct cardiac infection remains equivocal. In vitro studies show infection and replication within human pluripotent stem cell (hPSC)-derived cardiomyocytes [21, 22], while hPSC-smooth muscle cells remain uninfected [23]. Autopsies of 39 patients with COVID-19 detected SARS-CoV-2 negative sense RNA indicative of active viral replication in the myocardium of only five patients with the highest viral loads [24].
In autopsies of a further 41 patients, SARS-CoV-2+ cells in the myocardium were rare despite viral RNA being detected in 30 hearts [25]. Furthermore, smaller studies of autopsy specimens from five and eight COVID-19 patients failed to detect SARS-CoV-2 within the heart entirely, even when patients displayed severe myofibrillar anomalies [21, 26].
In IAV infection, it is equally uncertain whether early cardiomyocyte damage is linked primarily to virus presence or a secondary consequence of the immune response in IAV infection. IAV has been reported to replicate within hPSC-cardiomyocytes [27], and IAV or antigens have been found directly in the heart in mice [27, 28] and humans [29, 30] in small case studies.
One potential mechanistic disparity between influenza virus and SARS-CoV-2 induction of cardiac complications is the induction of an interferon (IFN) response in the heart. For example, 2 days post-IAV infection, the expression of IFN stimulated genes within the heart of IAV-infected mice was increased 50-fold in infected compared with uninfected mice [32].
In contrast, several studies have found that both respiratory and extra-respiratory type I IFN responses are significantly blunted during SARS-CoV-2 infection [33, 34]. For example, a Syrian hamster model of SARS-CoV-2 infection showed inhibited type I IFN responses in the respiratory tract despite a high burden of replicating virus, accompanied by inflammation in the heart, which also lacked type I IFN upregulation [35].
This may be attributable to SARS-CoV-2 production of proteins which suppress type I IFN release [36, 37]. The lack of efficient IFN induction by SARS-CoV-2 may be responsible for triggering the observed higher rate of cardiac complications than in more IFN-stimulatory seasonal IAVs [38, 39]. Indeed, several studies have shown that type I IFNs play a protective role in the development of cardiovascular diseases such as pathological hypertrophy and virally induced left ventricular dysfunction [40, 41]. However, this hypothesis remains to be confirmed.
Transcriptomic analysis of patient myocardial tissue offers a unique opportunity to understand the mechanisms of SARS-CoV-2 and IAV-induced cardiac complications. Specifically, spatial transcriptomics that consider intra-organ heterogeneity [42, 43], provide a powerful tool for characterizing host responses to respiratory viral infections outside of the respiratory tract.
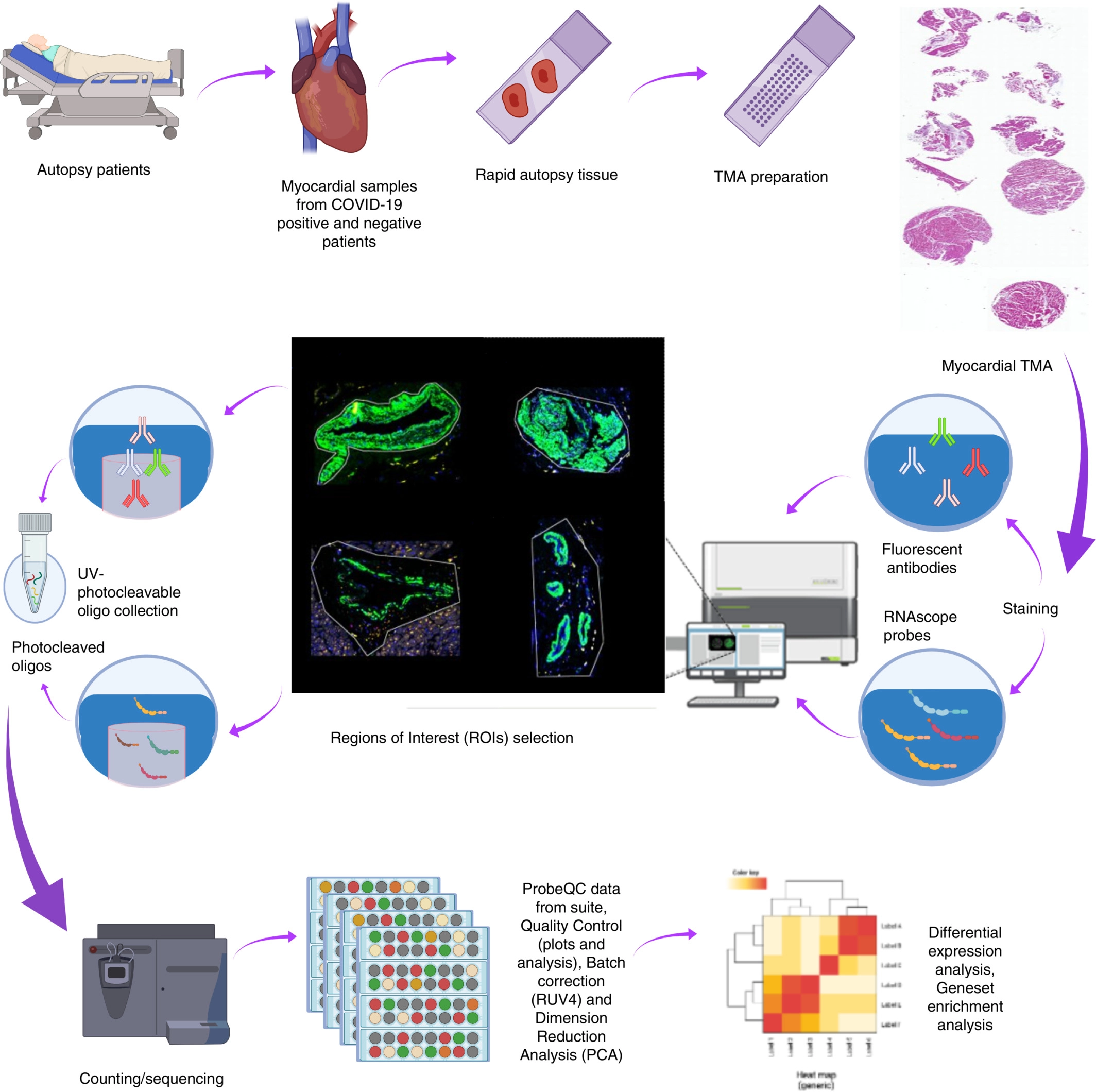
Here, we use targeted spatial transcriptomic characterization of myocardial tissue to generate an in-depth picture of the myocardial transcriptional landscape of COVID-19, pandemic H1N1 influenza and uninfected control patients and shed light on the mechanisms that might drive these different clinical outcomes (Figure 1).
Our study revealed that DNA damage pathways were enriched for in COVID-19 tissues, whereas pH1N1 elicited a more inflammatory response in cardiac tissues.



{kind=link}