











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Coronaviruses spread broadly among humans leading to a spectrum of respiratory diseases ranging from flu-like symptoms or pneumonia to acute respiratory distress syndrome, which caused high mortality in human populations.[2]
Therefore, the clinical deterioration and tissue damage during SARS-CoV-2 infection may result from a combination of direct virus-induced cytopathic effects and maladjusted immune responses. As described earlier, one of the clinical features of SARS-CoV-2 infection is the reduction of peripheral T cell subsets, as a unique characteristic in COVID-19 patients during acute infection.[4]
Recent data shed new light on the role of impaired immune response and eventual lymphopenia in SARS-CoV-2 pathogenesis.[5] Here, we provide a brief introduction to the immune response against SARS-CoV-2 and possible mechanisms underlying reduced peripheral T cell subsets in COVID-19 patients.
The Adaptive Immune Response
The adaptive immune response against viral infections began to develop exact and powerful protector immunity against viruses. The adaptive immune response to viral infections exerts through the effector function of cytotoxic T lymphocyte (CTL) response. CTLs are generated in response to intracellular invading pathogens, and they specifically recognize and kill virus-infected cells and/or release inhibitory antiviral-soluble factors. Thus, a pointy increase in CTL count is extremely expected in CTL patients with SARS-CoV-2 infection.[10]
However, unlike the traditional immune responses against viruses, in SARS-CoV-2 infection, a different response shaped which is accompanied by particular T cell lymphopenia, with a rapid decrease in both CD4 and CD8 T cell subsets. The latest report indicated the reduced number of CD4+ and CD8+ T cells within the peripheral blood of SARS-CoV-2-infected patients, similar to patients with SARS-CoV, with concomitant hyperactivated T cells shown by high proportions of CD4-restricted HLA-DR (3.47%) and CD38 (CD8, 39.4%) double-positive populations.[11]
Here, the possible factors that could be involved in the general reduction of peripheral T lymphocytes during SARS-CoV-2 are further discussed in detail [Figure 1].

Possible mechanisms involved within the reduction of peripheral lymphocyte subsets in patients with severe acute respiratory syndrome coronavirus 2. The nicotinamide adenine dinucleotide + depletion subsequent to poly-ADP-ribose polymerase 1 hyperactivation and CD38 overexpression leads to cell death and T cell depletion. Further, the negative effect of cytokines on T cells and virus-induced apoptosis could also be involved in severe acute respiratory syndrome coronavirus 2-related lymphopenia
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8977610/
Most COVID-19 patients display overt lymphopenia (Figure 1, top left), which is associated with CD4+ and CD8+ T cell activation and proliferation, cytokine serum levels increase (e.g., IL-1RA IL-6, IL-8, IL-10, and CXCL10), and T-bet+ with decreased CXCR5 B cells [1,3]. Hence, SARS-CoV-2 infection can trigger a complex crosstalk of the immune system.
The study findings were published in the peer reviewed Journal of Clinical Medicine.
https://www.mdpi.com/2077-0383/12/3/998
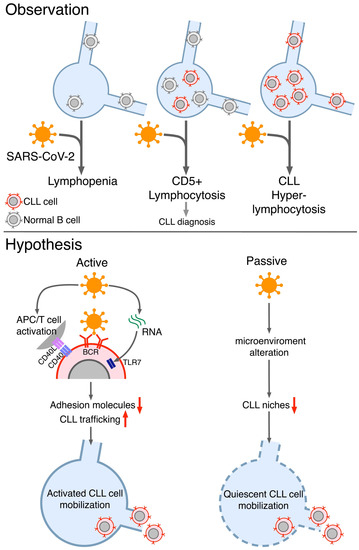
This complex and heterogeneous immune response to SARS-CoV-2 infection might be further exacerbated in patients with oncological malignancies whose immune system is compromised [5].
Chronic lymphocytic leukemia (CLL), the most commonB cell leukemia in adult Caucasians, is characterized by the expansion of a monoclonal population of CD5+ B lymphocytes. As of today, it is not fully clear whether SARS-CoV-2 infection in CLL patients leads, on average, to worse or milder COVID-19 symptomatology compared to age-matched healthy individuals or groups with other comorbidities.



{kind=link}
[…] Most COVID-19 patients display overt lymphopenia […]
[…] Most COVID-19 patients display overt lymphopenia […]