











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



While more than 32 million individuals in the U.S. have a documented penicillin allergy in their medical record, studies have shown that more 95 percent actually can be treated safely with this class of antibiotics, improving treatment outcomes and reducing the risk of infection with dangerous resistant pathogens such as Clostridium difficile (C. difficile).
A review article in the January 15 issue of JAMA recommends best practices for evaluation of reported penicillin allergies and provides clinicians with guidance and tools to help determine appropriate procedures based on the severity of previously reported reactions.
The report is the result of a collaboration among physicians at Massachusetts General Hospital (MGH), Kaiser Permanente, and Northwestern Medicine at Northwestern University.
Lead and corresponding author Erica Shenoy, MD, Ph.D., MGH Division of Infectious Diseases, and senior author Kimberly Blumenthal, MD, MSc, MGH Division of Rheumatology, Allergy and Immunology, have been addressing the issue of penicillin allergy evaluation for several years; and the current report is a result of a consensus development among the American Academy of Allergy, Asthma and Immunology; the Infectious Diseases Society of America, and the Society for Healthcare Epidemiology of America.
Shenoy explains that the common use of penicillin and related antibiotics called beta-lactams is behind the frequent documentation of penicillin allergy.
“Many reported penicillin allergies are established during childhood, when it is by far the most commonly prescribed antibiotic.
If a penicillin is prescribed for what is actually a viral rather than a bacterial infection, a rash that develops may be caused by the virus but attributed to a penicillin allergy, which then is documented in the patient’s chart and never questioned again.
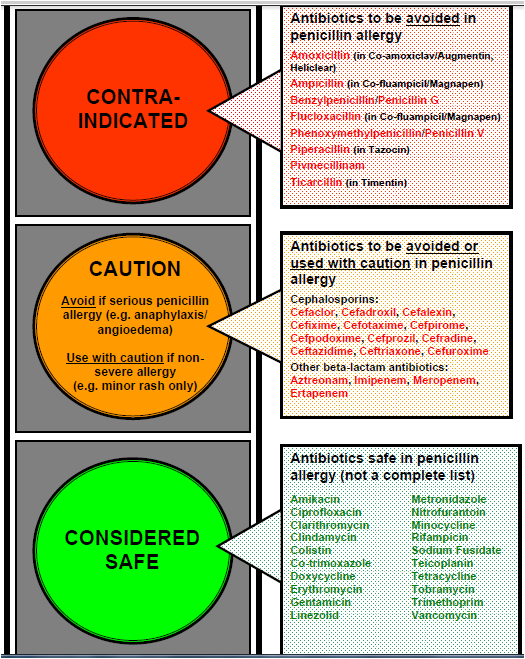
The allergy label can lead to patients’ not receiving penicillins and related drugs that are often the best drugs to either treat or prevent common infections.
When alternatives are used instead, these can lead to increased risk of treatment or prevention failure, as well as increased risk of C. difficile.”
Key to the recommendations of the team—which also includes Eric Macy, MD, MS, of Kaiser Permanente, San Diego, and Theresa Rowe, DO, MS, of Northwestern Medicine—is taking a comprehensive history of the reaction that led to allergy documentation, which can help determine the patient’s risk level and appropriate procedures for testing. Blumenthal says,
“A simple history can often distinguish intolerances—for example, headaches or nausea—from allergies.

Side effects should be judged by their severity and, after discussion with the patient, clinicians should consider the safety of a potential drug challenge.
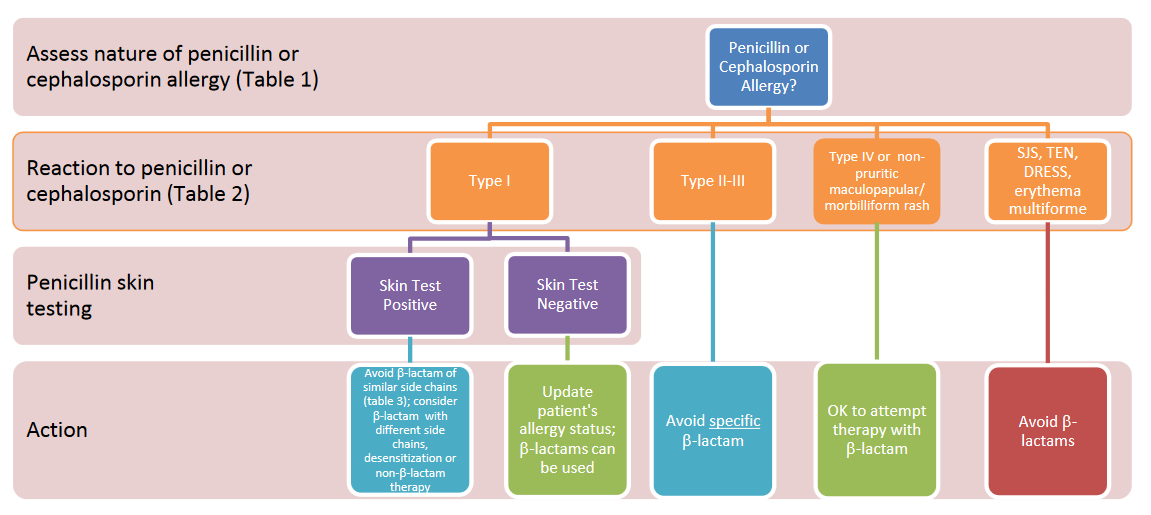
For patients whose symptoms—such as hives, shortness of breath, wheezing or anaphylaxis—suggest a true allergic reaction, this report provides guidance for evaluation, risk determination and allergy management.”
The authors stress that some form of evaluation of a documented penicillin allergy can and should be carried out in any clinical setting—from routine outpatient care to preparation for surgery or other procedures—and for all patients with such documentation, including children and pregnant women.
Shenoy says, “I can’t think of a clinical encounter in which a careful allergy history and then a planned course of action that may include penicillin skin testing, amoxicillin challenge or referral to an allergist would not be of benefit to the patient.
If I had my way, verification of a penicillin allergy would be on many of our checklists, just like age-related screenings and immunizations.
Evaluating a reported penicillin allergy, regardless of the current need for an antibiotic, can lead to really important benefits for our patients.”
Blumenthal adds, “It is my hope that all patients who believe they have a penicillin allergy—including the parents of children with a documented penicillin allergy—become aware that the allergy label may not be accurate, is not benign and can be evaluated further.
If such allergies are routinely evaluated, patients will not needlessly avoid the beta-lactams that may be the best treatment for their infection and reduce the development of antibiotic resistance.
Allergies to penicillin or to other drugs are very real, so it is important not to be cavalier about the process of allergy evaluation. When patients have an unclear or severe allergy history, allergists are available and uniquely qualified to help with the assessment.”
More information: JAMA (2019). DOI: 10.1001/jama.2018.19283
Provided by Massachusetts General Hospital



{kind=link}