











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The coronavirus variant detected in South Africa poses a “significant re-infection risk” and raises concerns over vaccine effectiveness, according to preliminary research Wednesday, as separate studies suggested the British strain would likely be constrained by immunisations.
Several new variants – each with a cluster of genetic mutations – have emerged in recent weeks, sparking fears over an increase in infectiousness as well as suggestions that the virus could begin to elude immune response, whether from prior infection or a vaccine.
These new variants, detected from Britain, South Africa and Brazil, have mutations to the virus’ spike protein, which enables the virus to latch onto human cells and therefore plays a key role in driving infections.
But it is one mutation in particular – known as E484K and present in the variants detected in South Africa and Brazil but not the one from Britain – that has experts particularly worried about immunity “escape”.
In a new study, which has not yet been peer reviewed, researchers in South Africa tested the variant found there – called 501Y.V2 – against blood plasma from recovered COVID-19 patients.
They found that it was resistant to neutralising antibodies built up from prior infection, but said more research was needed into the effectiveness of other parts of the immune response.
“Here we show that the 501Y.V2 lineage, which contains nine spike mutations and rapidly emerged in South Africa during the second half of 2020, is largely resistant to neutralising antibodies elicited by infection with previously circulating lineages,” the authors said.
“This suggests that, despite the many people who have already been infected with SARS-CoV-2 globally and are presumed to have accumulated some level of immunity, new variants such as 501Y.V2 pose a significant re-infection risk.”
The researchers added that this might also affect the use of convalescent plasma as a treatment for COVID-19. They also suggested it could have “implications” for vaccines developed based on immune responses to the virus’s spike protein.
Trevor Bedford of the Fred Hutchinson Research Center tweeted that this variant could “spread more widely in the coming months”.
If the results of the South African study are confirmed, he said it may be necessary to adapt the virus “strain” used in developing the vaccine by autumn of this year.
The findings are “not good news but it’s not unexpected,” said James Naismith, Director of the Rosalind Franklin Institute, in comments to the Science Media Centre.
He said real world immune responses were more complex than those of the blood plasma neutralising antibodies.
“The vaccines do stimulate very strong responses, immunity is a sliding scale, it’s not an on/off switch,” he added.
UK strain
Two other preliminary studies posted online on Wednesday found that the antibodies from previously-infected patients are largely effective against the variant detected in Britain and that the BioNTech/Pfizer vaccine appears to be guard against it as well.
Researchers said their early findings into the fast-spreading strain, known as B.1.1.7, suggested that the variant would not be able to evade the protective effect of current vaccines.
“Our results suggest that the majority of vaccine responses should be effective against the B.1.1.7 variant,” concluded researchers from Britain and the Netherlands in one of the studies.
The authors tested the UK strain in the laboratory with antibody-rich blood plasma from 36 patients who had recovered from either mild or severe forms of COVID-19 and found most were able to neutralise the variant.
A separate study by researchers from BioNTech and Pfizer compared the neutralising effect of plasma from 16 participants in their vaccine clinical trials against the British variant and the original virus that emerged in Wuhan, China.
They concluded it was “unlikely” the B.1.1.7 variant could escape the immune protection of the vaccine.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), has resulted in substantial morbidity and mortality worldwide1,2. Infected individuals develop neutralizing antibodies that can persist for months3–5.
Neutralizing antibodies are considered the primary correlate of protection against reinfection for most vaccines, including SARS-CoV-26,7, and are being actively pursued as therapeutics8,9.
The SARS-CoV-2 receptor binding domain (RBD) is the dominant target of the neutralizing response during infection7,10-13. Consequently, the overwhelming majority of monoclonal neutralizing antibodies isolated thus far from infected individuals, immunoglobulin libraries, or immunized animal models, target this region10,11,13,14.
These antibodies can be broadly divided into four main classes15, of which class 1 and class 2 antibodies target site I10 epitopes that overlap with the angiotensin converting enzyme 2 (ACE2) receptor binding site. Class 1 antibodies are most frequently elicited by SARS-CoV-2 infection and are comprised almost entirely of immunoglobulin V-gene (VH3-53/66) germline restricted antibodies, forming a multi-donor class with highly similar epitopes only accessible in the RBD ‘up’ conformation11,15,16.
Class 2 antibodies also bind to site I10,15, but can bind to both RBD ‘up’ and RBD ‘down’ conformations of spike. Although they can use a more diverse VH-gene pool, class 2 antibodies include VH1-2 germline restricted antibodies that form a second commonly elicited multi-donor class of public antibodies17. The RBD is also the target of several nanobodies/sybodies that are being considered for clinical development18,19.
After the RBD, the N-terminal domain (NTD) of spike is the next most frequently targeted by neutralizing antibodies, and several potent monoclonal antibodies to this region also being considered for clinical development20–22. Remarkably, despite being derived from diverse VH-genes, almost all these antibodies target a single immunodominant site on NTD, involving the N1-loop (NTD N-terminus), N3-loop (supersite β-hairpin), and N5-loop (supersite loop). A subset of these antibodies also forms a third multi-donor class, with a common VH1-24 germline restricted mode of spike recognition.
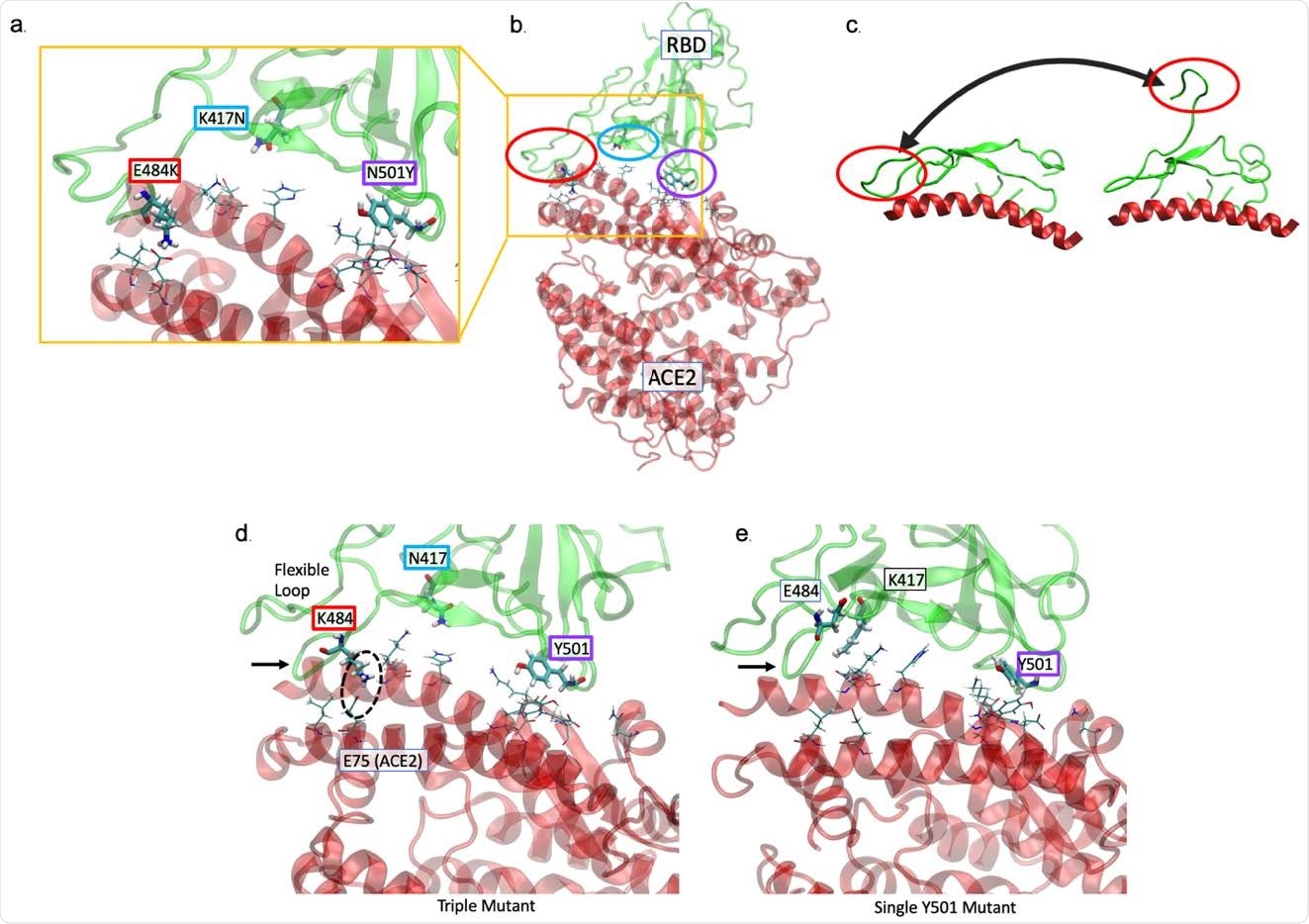
We, and others, recently described the emergence of a new SARS-CoV-2 lineage in South Africa, 501Y.V2, that included nine changes in the spike protein. These can be divided into two subsets, one cluster in NTD that includes four substitutions and a deletion (L18F, D80A, D215G, Δ242-244, and R246I), and another cluster of three substitutions in RBD (K417N, E484K, and N501Y).
Although the 501Y change has been associated with increased transmissibility, rather than immune pressure, the accumulation of mutations specifically within these two immunodominant regions of spike is highly suggestive of escape from neutralization. Indeed, mutations at 484 have been shown to reduce neutralization sensitivity23,24.
Furthermore, mutations in these same regions have also been described in a new variant, which has recently emerged independently in Brazil25. Lastly, variants in the UK and USA, albeit with fewer potential antibody escape mutations have also been described, suggesting the global emergence of new SARS-CoV-2 variants26.
Here we show that spike mutations in the 501Y.V2 lineage confer neutralization escape from multiple classes of SARS-CoV-2 directed monoclonal antibodies. Furthermore, we observe significantly increased neutralization resistance of 501Y.V2 to plasma from individuals previously infected with SARS-CoV-2, with implications for both rates of re-infection, and vaccine effectiveness.
Discussion
SARS-CoV-2, the virus responsible for the COVID-19 pandemic is evolving, with new lineages being reported all over the world. Amongst previous lineages, D614G was shown to have faster growth in vitro, enhanced transmission in small animals, and has subsequently become globally dominant28–30.
N501Y has been shown to increase affinity for the human ACE2 receptor, which together with the repeated and independent evolution of 501Y containing lineages25,26,31, strongly argues for enhanced transmissibility of these new variants. Here we show that the 501Y.V2 lineage, that contains nine spike mutations, and rapidly emerged in South Africa during the second half of 2020, is largely resistant to neutralizing antibodies elicited by infection with previously circulating lineages.
This suggests that, despite the many people who have already been infected with SARS-CoV-2 globally and are presumed to have accumulated some level of immunity, new variants such as 501Y.V2 pose a significant re-infection risk.
While higher titres of neutralizing antibodies are common in hospitalized individuals, however most SARS-CoV-2 infected people develop moderate neutralization titres3–5. Therefore, the data herein suggest that most individuals infected with previous SARS-CoV-2 lineages will have minimal or no detectable neutralization activity against 501Y.V2.
This dramatic effect on plasma neutralization can be explained by the dominance of RBD-directed neutralizing antibodies10,11,13. These data are supported by studies showing reduced plasma neutralization titres mediated by the E484K change alone23,24.
Importantly, here we show that the K417N change also has a crucial role in viral escape, effectively abrogating neutralization by a well-defined, multi-donor class of VH3-53/66 germline restricted public antibodies that comprise some of the most common and potent neutralizing antibodies to SARS-CoV-211,17.
The marked loss of neutralization against 501Y.V2 compared to the RBD-only chimeric virus demonstrates the important role that mutations in the NTD play in mediating immune escape. While the L18F change (found in 501Y.V2) has previously been linked to neutralization resistance22, we also define an important role for a relatively small, three amino acid deletion in the 501Y.V2 NTD domain that completely disrupts a dominant public antibody response to the N5-loop supersite20–22. This deletion predominates among 501Y.V2 variants, and occurs either alone or with an R246I substitution that has also been shown to abrogate neutralization by several NTD-directed neutralizing antibodies22.
A recently identified lineage in Brazil also has changes at key positions shown here to affect neutralizing antibodies (417T, 484K in RBD and 18F, 20N in NTD – the last mutation adding a glycosylation sequon)25. Our data suggest that this lineage is also likely to exhibit significant levels of neutralization resistance, making both lineages of considerable public health concern.
The independent emergence and subsequent selection for two distinct 501Y lineages with key mutations conferring neutralization resistance strongly argues for selection by neutralizing antibodies as the dominant driver for SARS-CoV-2 spike diversification.
The relatively rapid acquisition of a comprehensive suite of neutralization escape mutations likely occurred because of the large number of commonly shared public antibodies (eg: VH3-53/66, VH1-2, VH1-24) to both the RBD and NTD of spike, together with high levels of SARS-CoV-2 transmission around the world.
The sporadic emergence of escape mutations in long-term viral shedders, including immunocompromised individuals, may also contribute to the emergence of neutralization resistant viruses32. Altogether, these data highlight the need for increased, ongoing surveillance and sequencing during the SARS-CoV-2 pandemic.
Crucially, it is from these same public antibody responses that many therapeutic strategies currently under development have been derived8,9,33. The overwhelming majority of monoclonal antibodies already on the path to licensure target residues K417 or E484 and will therefore be ineffective against 501Y.V2.
Amongst these antibodies, some have already been granted emergency use authorization in the USA (Regeneron Pharmaceuticals and Eli Lilly and Company). In addition, a next generation of potent neutralizing antibodies that target the NTD N5-loop supersite have been suggested for clinical development but are also likely to be futile against 501Y.V2.
These data also have implications for the effectiveness of SARS-CoV-2 vaccines, which are principally based on immune responses to the spike protein. Neutralizing antibodies have repeatedly been demonstrated as the primary correlate of protection for most vaccines, including those designed to prevent infection with respiratory pathogens34.
Despite neutralization escape, we show here that a significant proportion of non-neutralizing, RBD binding antibodies remain active against 501Y.V2. While antibody effector functions elicited by infection and vaccination have been implicated in protecting from reinfection and disease35,36, the role of non-neutralizing antibodies and the efficacy of T cell responses to 501Y.V2 remain to be elucidated.
Ultimately, the correlates of protection against SARS-CoV-2 infection and severe COVID-19 disease remain undetermined and rely upon ongoing large-scale clinical trials. Nevertheless, the speed and scope of 501Y.V2 mediated immune escape from pre-existing neutralizing antibodies highlight the urgent requirement for rapidly adaptable vaccine design platforms, and the need to identify less mutable viral targets for incorporation into future immunogens.
reference link: https://www.biorxiv.org/content/10.1101/2021.01.18.427166v1.full
Dr Julian W Tang, Honorary Associate Professor/Clinical Virologist at the University of Leicester, said:
“The South African variant (B.1.351 or 501Y.V2) differs significantly from the UK B.1.1.7(variant) in several ways that may impact on vaccine effectiveness.
“Both variants share the N501Y mutation in the viral S gene which lies in the receptor binding domain (RBD) – where the virus binds to the host cell – and where vaccine-induced antibodies bind to the virus. But the South African variant has two more mutations – E484K and K417N – in this RBD region that are absent in the UK variant. These two additional mutations may interfere more with vaccine effectiveness in the South African variant than in the UK variant.
“This does not mean that the existing COVID-19 vaccines will not work at all, just that the antibodies induced by the current vaccines may not bind and neutralise the South African variant as well as it would the other circulating viruses – including the UK variant.
“Even if the South African variant becomes more widespread and dominant, the mRNA (Pfizer-BioNTech and Moderna) and adenovirus-vectored (Oxford-Astrazeneca and Russian Sputnik V) vaccines can be modified to be more close-fitting and effective against this variant in a few months.
“Meanwhile, most of us believe that the existing vaccines are likely to work to some extent to reduce infection/ transmission rates and severe disease against both the UK and South African variants – as the various mutations have not altered the S protein shape that the current vaccine induced antibodies will not bind at all.”
Prof Francois Balloux, Professor of Computational Systems Biology and Director, UCL Genetics Institute, University College London, said:
“The ‘South African variant’ carries a mutation in the spike protein called E484K, which is not present in the ‘UK strain’. The E484K mutation has been shown to reduce antibody recognition. As such, it helps the virus SARS-CoV-2 to bypass immune protection provided by prior infection or vaccination. It is not anticipated that this mutation is sufficient for the ‘South African’ variant to bypass the protection provided by current vaccines. It’s possible that new variants will affect the efficacy of the covid vaccines, but we shouldn’t make that assumption yet about the South African one.”
Prof Lawrence S. Young, Virologist and Professor of Molecular Oncology, Warwick Medical School, University of Warwick, said:
“The South African virus variant was recently reported in a preprint ahead of formal publication. The variant has multiple spike mutations and emerged in a major metropolitan area in South Africa following the first wave of the epidemic and then spread to multiple locations within two other neighbouring provinces. It has rapidly spread become the dominant virus variant in the Eastern and Western Cape provinces.
“The South African variant has 3 mutations at key sites in the receptor binding domain (K417N, E484K and N501Y) of the spike gene. Two of these (E484K and N501Y) are within the receptor-binding motif (RBM), the main functional motif that forms the interface with the human ACE2 receptor.
The N501Y mutation is the same as that found in the UK virus variant. These changes are consistent with both these variants being more infectious (transmissible) but we don’t know whether they will affect the disease severity. While changes in the UK variant are unlikely to impact the effectiveness of current vaccines, the accumulation of more spike mutations in the South African variant are more of a concern and could lead to some escape from immune protection.
“Variants of SARS-CoV-2 have been around since the beginning of the pandemic and are a product of the natural process by which viruses develop and adapt to their hosts as they replicate. Most of these mutations have no effect on the behaviour of the virus but very occasionally they can improve the ability of the virus to infect and/or become more resistant to the body’s immune response.
Many thousands of these mutations have already been identified in isolates of the virus with around 4000 spike mutations being found in different viruses from around the world. The UK and South African virus variants have changes in the spike gene consistent with the possibility that they are more infectious.
“But the standard measures to restrict transmission (hands, face, space) will prevent infection with this variant. Along with improved surveillance (testing, tracing and isolating) and expediating the roll out of the vaccine, these measures will prevent transmission of this variant and any others that will arise.
“The move to harsher levels of restriction across the country is inevitable. It is essential that we do everything possible to prevent the South African variant from spreading to the UK population. Quarantine measures and restricting travel from and to South Africa are imperative.”
Dr Simon Clarke, Associate Professor in Cellular Microbiology at the University of Reading, said:
“The variant found in South Africa which is now also seen in the UK, is another mutated version of the coronavirus which is causing significant problems.
“The South African variant has a number additional mutations including changes to some of the virus’ spike protein which are concerning. They cause more extensive alteration of the spike protein than the changes in the Kent variant and may make the virus less susceptible to the immune response triggered by the vaccines.
“While it is more infectious, it currently remains unclear whether it causes a more severe form of the disease. Moreover, the South African variant is a more difficult virus to track as it lacks some mutations in the spike found in the Kent virus which make it easily detectable by the PCR test used by the NHS.”
Prof James Naismith, Director of the Rosalind Franklin Institute, and University of Oxford, said:
“Viruses mutate and new strains will emerge. The so-called South African strain has a number of changes, and scientists are working flat out to understand their significance. Some of the changes are quite significant and thus scientists are paying a lot of attention. We do not yet know enough to say more than this.
“For the general public, I would say think about our human nature. Many of us like a good scare and horror stories are part and parcel of human culture, which means such things get a lot of coverage. However a drumbeat of nightmare scenarios about this new variant does nothing but create anxiety because too little is known and there is nothing we can do about it at the moment. Prolonged anxiety is far from enjoyable and leads to mental illness. I would say there are many much more positive things we can do.
“We can support scientists to work on the new variants and keep other research efforts to treat the disease going (don’t stop funding covid19 science just yet). We can all help if we redouble our efforts to wash our hands, wear a mask and socially distance.
The faster and further the vaccine is rolled out, the quicker the end to this nightmare. We can all help each other through kindness and understanding, many are grieving, others are financially very stretched and other are very lonely. We can help by not amplifying or spreading doomsday scenarios or spreading magical thinking or nonsense information.
“And we need to have a proper informed debate: further social restrictions are required if we wish to avoid overloading the NHS before the vaccines stop spread. Those who advocate reducing social restrictions really should make clear the costs in lives of their policy. In our democracy we elect politicians, not scientists, to take decisions. We expect politicians to make decisions based on facts, not fantasy.”
reference link: https://www.sciencemediacentre.org/expert-reaction-to-the-south-african-variant/



{kind=link}