








 Competitive Coexistence: Post-War Strategic Outlook")

 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



You might have already heard this recommendation, but researchers have now found an additional reason why three-layered masks are safer than single or double-layered alternatives.
While this advice was originally based on studies that showed three layers prevented small particles from passing through the mask pores, researchers have now shown that three-layered surgical masks are also most effective at stopping large droplets from a cough or sneeze from getting atomized into smaller droplets.
These large cough droplets can penetrate through the single- and double-layer masks and atomize to much smaller droplets, which is particularly crucial since these smaller droplets (often called aerosols) are able to linger in the air for longer periods of time. Researchers studied surgical masks with one, two and three layers to demonstrate this behavior.
The researchers reported their results in Science Advances on March 5.
The team notes that single and double-layer masks do provide protection in blocking some of the liquid volume of the original droplet and are significantly better than wearing no mask at all.
They hope their findings on ideal mask pore size, material thickness, and layering could be used by manufacturers to produce the most effective masks designs.
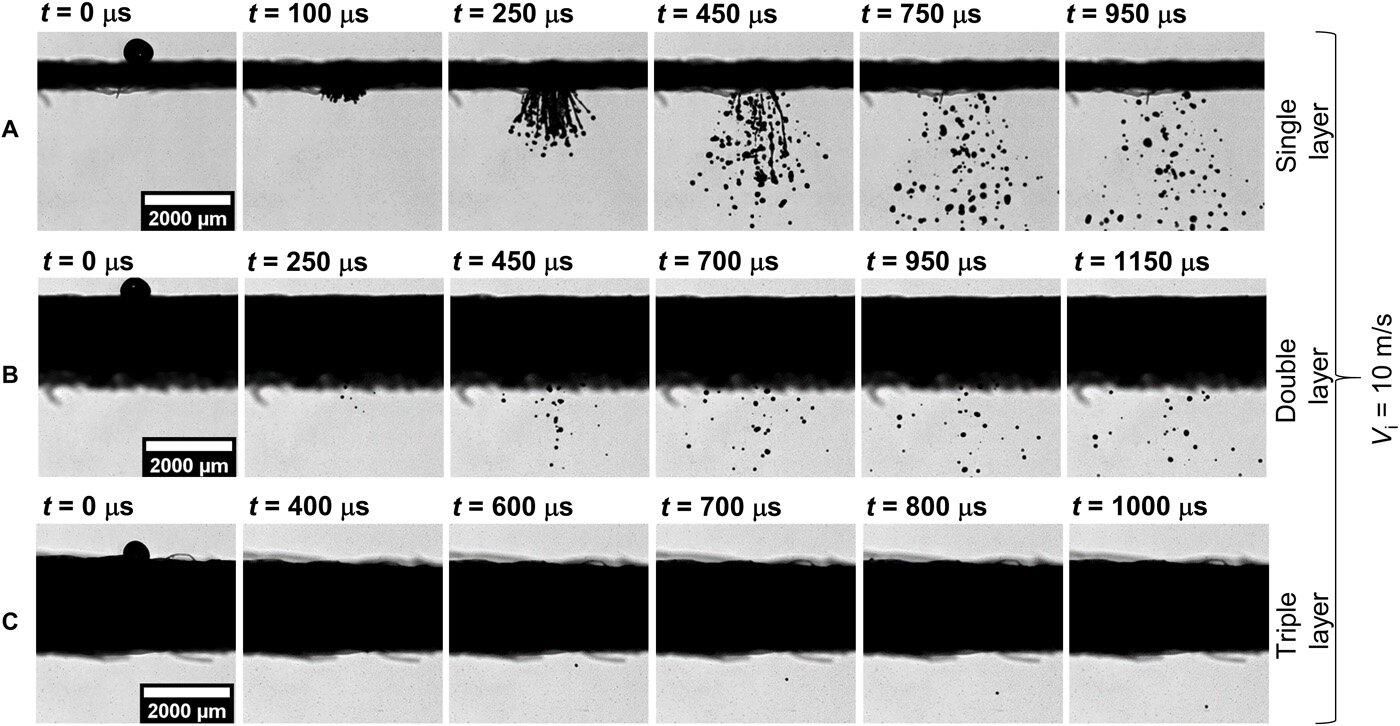
Using a droplet generator and a high-speed time-lapse camera, the team of engineers from the University of California San Diego, Indian Institute of Science and University of Toronto found that, counterintuitively, large respiratory droplets containing virus emulating particles (VEPs) actually get atomized when they hit a single-layer mask, and many of these VEPs pass through that layer.
Think of it like a water droplet breaking into smaller droplets as it’s being squeezed through a sieve.
For a 620 micron droplet – the size of a large droplet from a cough or sneeze – a single-layer surgical mask only restricts about 30 percent of the droplet volume; a double-layer mask performs better, restricting about 91 percent of the droplet volume; while a three layer mask has negligible, nearly zero droplet ejection.
“While it is expected that large solid particles in the 500-600-micron range should be stopped by a single-layer mask with average pore size of 30 micron, we are showing that this is not the case for liquid droplets,” said Abhishek Saha, professor of mechanical and aerospace engineering at UC San Diego and a co-author of the paper.
“If these larger respiratory droplets have enough velocity, which happens for coughs or sneezes, when they land on a single-layer of this material it gets dispersed and squeezed through the smaller pores in the mask.”
This is a problem. Droplet physics models have shown that while these large droplets are expected to fall to the ground very quickly due to gravity, these now smaller, 50-80 micron-sized droplets coming through the first and second layer of a mask will linger in the air, where they can spread to people at larger distances.
The team of engineers – which also includes Professors Swetaprovo Chaudhuri from University of Toronto, and Saptarshi Basu of the Indian Institute of Science – were well-versed in this type of experiment and analysis, though they were used to studying the aerodynamics and physics of droplets for applications including propulsion systems, combustion, or thermal sprays.
“We do droplet impact experiments a lot in our labs,” said Saha. “For this study, a special generator was used to produce a relatively fast-moving droplet. The droplet was then allowed to land on a piece of mask material—that could be a single layer, double, or triple layer, depending on which we’re testing. Simultaneously, we use a high-speed camera to see what happens to the droplet.”
Going forward, the team plans to investigate the role of different mask materials, as well as the effect of damp or wet masks, on particle attrition.
Emerging and reemerging infections have emerged as a threat to human health in recent decades [1]. Given how interconnected the world is today, a pathogen capable of human-to-human transmission can spark an outbreak far from where it originated. The virus causing the Middle East Respiratory Syndrome, for example, emerged in the Middle East but caused an outbreak in Korea.
The world is in the midst of the COVID-19 pandemic, which is caused by the SARS-CoV-2 virus. Lockdowns and travel restrictions imposed to halt the spread of COVID-19 have led to devastating economic repercussions. The control of an infectious disease is based on knowledge of its mode of transmission.
The recent COVID-19 pandemic is caused by the novel coronavirus, SARS-CoV-2, which is transmitted largely by the respiratory route (vide infra) [2, 3].
The best nonpharmaceutical interventions against disease spread via the respiratory route are broadly termed social or safe distancing measures, i.e., reducing close contact between individuals [4, 5]. Where safe distancing is not possible, personal protective equipment (PPE) is the accepted mode of self-protection.
Masks and respirators are arguably the most important piece of PPE. They are a physical barrier to respiratory droplets that may enter through the nose and mouth and to the expulsion of mucosalivary droplets from infected individuals [6, 7]. Their role may be particularly important in COVID-19, where infected individuals may be shedding virus while asymptomatic or presymptomatic [8–10].
There are many different types of face masks and respirators offering different levels of protection to users [11–15]. Generally, masks do not fit tightly while respirators do. Masks and respirators may be reusable or disposable. Reusable ones include industrial-use half or full facepiece respirators with cartridge filters attached and homemade or commercial cloth masks; disposable ones include surgical masks, N95 respirators, and KN95 respirators.
They all serve the general purpose of providing some form of protection against contaminants in the air, ranging from pollen to chemical fumes to pathogens. The filtering capacity, and hence the level of protection against pollutants and pathogens, depends on the materials used and the engineering design [11–15].
Contaminants in the air differ vastly in size (Figure 1). SARS-CoV-2 has a size ranging from 60 to 140 nm [16], smaller than bacteria, dust, and pollen. Therefore, masks and respirators made of materials with larger pore sizes, such as cotton and synthetic fabric, will not be able to effectively filter these viruses or tiny virus-laden droplets, as compared with those made of materials with much smaller pore sizes.
Likewise, masks and respirators made of or coated with water-resistant materials are more effective against large virus-laden respiratory droplets and fluid spills. In addition to filtering capacity, factors such as user comfort and breathability also vary across different models.
For instance, although the tight-fitting N95 respirator has filtering capacity superior to surgical masks, they have lower breathability and may cause discomfort after hours of wearing.

Relative size chart of common airborne contaminants and pathogens.
Mask-wearing can be effective in the containment of communicable diseases [17, 18] and has thus become a new normal in many societies in the COVID-19 pandemic. The surge in demand for surgical masks and respirators has led to a global shortage of supply and raw materials. As a result, many people have resorted to making their own masks, recycling used masks, or settling for masks offering less protection than actually needed.
Researchers and industry players have therefore been working hard to address the issue of shortage, as well as to enhance the protection afforded by existing mask models.
These efforts include
- (i) sourcing and engineering alternative materials with sufficient filtering capacity,
- (ii) engineering the design of masks and respirators for better protection, breathability, and user comfort,
- (iii) developing and engineering multifunctional masks and materials with hydrophobic, antimicrobial, self-disinfecting, and even sensing properties, and
- (iv) exploring new technologies for efficient production and customization of masks, e.g., 3D printing [19].
Attempts to enhance the mask will pivot on understanding the basics of mask technology.
The fundamental questions, to our mind, are as follows:
- (i) how do masks (and the mask materials) protect us from pathogens;
- (ii) what are the existing models and materials of mask available in the market;
- (iii) how do they perform and how is their performance benchmarked against others;
- (iv) what are their limitations;
- (v) how can their performance be improved;
- (vi) what are some new features that can be incorporated into existing materials and models?
This review seeks to address the above questions.
How Do Masks Protect Us against Airborne Diseases
The Respiratory Route of Transmission
A respiratory pathogen may be transmitted via three routes—contact, droplet, and airborne spread [20]. Contact transmission may be direct (i.e., transfer of virus via contaminated hands) or indirect (i.e., via fomites) [20]. Fomites are objects or materials that may carry infection, and spread by fomites means spread by touch. Viruses do survive for some time on inanimate objects, although the viral load declines dramatically [21].
If we touch a contaminated surface and then touch our eyes or nose, we may inoculate the virus into our mucosal surfaces. The role of touch in the spread of a respiratory virus is best exemplified by studies of the Respiratory Syncytial Virus (RSV) [22, 23]. The spread of SARS-CoV-2 via fomites has been elegantly demonstrated by real-world contact tracing, aided by closed-circuit cameras [24].
Droplet spread and airborne spread are different modes of transmission of the virus through the air. Viruses released when an infected person coughs, sneezes, sings, talks, or merely exhales may be found in particles of varying sizes [17]. Generally, particles larger than 5 μm were thought to fall to the ground within 1 metre. More recently, however, the “gas cloud” hypothesis has been proposed [25].
Coughing, sneezing, or even exhaling produces mucosalivary droplets that exist as part of a cloud that “carries within it clusters of droplets with a continuum of droplet sizes” [25]. In combination with environmental factors, the “cloud” may be propelled up to 7–8 m. Wind speed, in particular, has been shown to play a role in determining the distance travelled by these particles [26].
Airborne spread occurs with pathogens found in exhaled droplets < 5 μm in diameter. These particles remain afloat for some time and are able to travel long distances. Respiratory viruses accepted as being capable of spread via the airborne route include measles and varicella zoster (chickenpox).
These viruses have a large R0, a feature thought to characterise spread by the airborne route. Interestingly, influenza, coronavirus, and rhinovirus RNA, generally thought to be transmitted by the droplet route, can be found in exhaled particles smaller or larger than 5 μm [17, 27].
Further, viable influenza is present in particles smaller than 5 μm. Hence, even viruses thought to be transmitted primarily by the respiratory droplet route may have the potential for airborne spread. Concern that SARS-CoV-2 may spread by the airborne route rose when it was shown to be viable for 3 hours in a drum that artificially kept particles afloat for several hours [21].
It might be less well known that more basic processes like talking can also lead to the release of potentially infectious droplets and aerosols. Using laser light scattering, it was found that there were average emissions of about 1000 droplet particles per second during speech, with high emission rates of up to 10,000 droplet particles per second [28].
By fitting the time-dependent decrease in particle detected to exponential decay times, the droplet particle sizes and estimated viral load could be calculated. The authors estimate that 1 min of loud speaking generates greater than 1000 droplets containing viruses [29].
Alternatively, respiratory particles of between 0.5 μm and 5 μm could be imaged by aerodynamic particle sizing. When participants made the “Aah” sound, there were emissions of up to 330 particles per second [30]. Taking into account that aerodynamic particle sizing measures particles under the detection limit of laser light scattering, these two methods can be seen to be complementary, and the total number of particles emitted could be even higher.
In a separate study, droplet particle emission was shown to be directly proportional to loudness, with the number of particles emitted increasing from 6 particles per second when whispering to 53 particles per second at the loudest talking. The number of particles generated varied greatly across individuals, raising the possibility of superspreaders who could be the primary spreaders of viruses by talking [31].
Mechanistic Effect of Wearing a Mask
Masks and other PPE items serve as a physical barrier to respiratory droplets. With imaging using laser light scattering, it was found that the number of flashes, which corresponds to the number of respiratory droplets, could be kept at background levels by covering the speaker’s mouth with a slightly damp washcloth [28].
An in vitro model with source and receiver mannequins was created to test the effect of the mask on filtering away radiolabelled aerosol emitted from the source. Masking at the source mannequin was consistently more effective at lowering radio-labelled aerosols reaching the receiver mannequin, whereas the only experimental setup where the receiver mannequin could be equally well protected was if the receiver mannequin wore an N95 mask sealed with Vaseline [32]. Therefore, masks can act as a physical barrier and seem to be more effective when worn by the droplet emitting person.
Masks have generally shown an effect in reducing virus emission from infected patients. The surgical mask was tested for its ability to block the release of various viruses by studying the amount of virus present in the exhaled breath of patients. The investigators were able to collect particles separated by size (> or <5 μm).
A significant drop in coronaviruses in both larger and smaller particles was observed with the mask on. The mask reduced influenza viruses found in larger but not smaller particles. After wearing a mask, no coronavirus was detected in all 11 patients, while influenza was detected in 1 patient’s respiratory particles (out of 27).
The mask did not lower rhinovirus counts in larger or smaller particles [17]. This suggests that surgical face masks can reduce the release of coronavirus and influenza from an infected person. In an earlier study for influenza, participants were induced to cough, and with both surgical masks and N95 masks, there was no influenza that could be detected by reverse transcriptase-polymerase chain reaction (RT-PCR) for 9 infected patients [33].
When the exhaled influenza virus was separated into the fractions based on size, it was found that surgical masks were highly effective at removing influenza from the larger coarse fraction (≥5 μm) but less effective from the fraction with smaller particles [34].
Wearing masks has also been shown to protect individuals coming into contact with an infected person. In a survey of 5 hospitals in Hong Kong during SARS, hospital staff were asked about the protective measures they took and this information was correlated with whether they were infected by SARS.
It was found that wearing masks was the single most important protective measure in reducing the chance of getting infected (p = 0.0001), and the people who wore either surgical masks or N95 masks were not among the 11 infected staff. There were however 2 instances of people who wore paper masks being infected, suggesting that the type of masks was also important [35].
A study compared the effectiveness of N95 and surgical face masks against viral respiratory infections in healthcare workers. Healthcare workers had no significant difference in influenza infection outcomes when wearing N95 and surgical masks, suggesting that both types of medical masks could protect similarly [36].
A meta-analysis was performed on clinical studies to explore the protective effect of masks. The risk ratio was calculated for the incidence of infection in the protected group vs. the unprotected group, where risk ratio < 1 suggests a reduced risk. Wearing a mask protected individuals against influenza-like illness, showing a risk ratio of 0.34, with a 95% confidence interval between 0.14 and 0.82. Similar to the study above, surgical masks and N95 masks showed little difference in protection, with a risk ratio of 0.84 and a 95% confidence interval of 0.36-1.99 suggesting no significant difference in risk [37].
Recently, a modelling study performed by Eikenberry et al. based on COVID-19 infection data obtained in New York and Washington suggested that the broad adoption of face mask by the general public can significantly reduce community transmission rate and death toll [18].
As shown in Figure 2, based on data obtained from 20th February to 30th March, the cumulative death rate was projected to be reduced to a greater extent as more people wear masks over the next 2 months. Therefore, the study concludes that community-wide adoption of face mask has great potential to help curtail community transmission and the burden of the COVID-19 pandemic.

Simulated future (cumulative) death tolls for Washington state, using either a fixed (top panels) or variable (bottom panels) transmission rate, β, and nine different permutations of general public mask coverage and effectiveness. The y-axes are scaled differently in the top and bottom panels. Reproduced with permission from Ref. [18]. Copyright 2020, Elsevier B.V. on behalf of KeAi Communications Co., Ltd.
Advantages and Caveats of Wearing Masks
Mask usage, in addition to other nonpharmaceutical interventions, can be an effective containment measure in an epidemic. Face masks can prevent dispersal of droplets when infected persons talk, sing, cough, or sneeze. The rate of emission of particles correlates with voice loudness during speech or other vocal activities [38].
A physical obstruction that prevents the wearer from touching the face, a mask may lead to better hand hygiene [24]. The reverse is also true—an increased tendency for wearers to touch their faces, such as when adjusting their masks [39]. Even with the right mask, wearers can still be infected if droplets enter via the eyes, thus highlighting the importance of additional protection [40].
Masks also reduce the risk of environmental contamination by respiratory droplets [24]. As mentioned, SARS-CoV-2 transmission via fomites has been documented [24]. In reality, usage by each individual varies. The mask may not fully cover the mouth and nose, or it may be used and reused too frequently.
These can mean huge variations in mask performance outcomes [24, 41]. In addition, wearers should avoid touching their faces and the external surface of their masks. Hand hygiene also varies from person to person. Hence, mask usage must be complemented by other behavioral changes for effective infection prevention.
Finally, the universal use of face masks prevents discrimination of individuals who wear masks when unwell because everybody is wearing a mask. Universal mask-wearing can create new social norms, motivating individuals to wear masks at the initial onset of symptoms without fear of being stigmatized.
The unintentional infection of healthy individuals by asymptomatic and presymptomatic persons can be avoided [39, 40]. Masks are visible indicators of crisis mode, which can prompt behavioral changes such as social distancing and frequent handwashing [39].
Complications of Asymptomatic and Presymptomatic Transmission
In the early stages of the COVID-19 pandemic, many countries did not recommend mask-wearing by healthy people to prevent panic buying and stockpiling [41]. Such paranoia can lead to a drastic shortage of medical masks for healthcare workers. The efficacy of masks in protecting individuals from being infected was also doubted.
Since then, governments, such as Singapore’s, have made it mandatory to wear a mask in public [42]. Such a change of policy direction has come about primarily because of increasing recognition of the concept of asymptomatic and presymptomatic transmission.
There has been a rise in asymptomatic and presymptomatic cases reported in many parts of the world. In an early example of such transmission, five symptomatic patients contracted the virus from one asymptomatic relative who travelled from Wuhan to Anyang [43].
In the same time period, another family cluster of three travelling from Wuhan to Guangzhou revealed asymptomatic transmission [44]. While the adult male presented clinical symptoms, his wife and son were both asymptomatic. All three tested positive for COVID-19 on RT-PCR.
A separate study on 82 residents at a long-term care skilled nursing facility revealed that out of the 30.3% positive cases, 43.5% were symptomatic while more than half were asymptomatic [45]. After 1 week, this asymptomatic group was reassessed and 10 out of 13 developed symptoms, leading to their reclassification as presymptomatic. Likewise in Singapore, 243 cases comprising of seven clusters could be explained by presymptomatic transmission [38].
In four of these clusters, the exact date of transmission could be determined to lead to the conclusion that transmission occurred 1-3 days before symptoms appear in the source patient. These cases demonstrate that viral shedding can occur prior to the onset and absence of symptoms, thus complicating the containment of this COVID-19 pandemic. Various governments have to enforce social distancing, good hygiene practices, and mask usage to effectively contain asymptomatic and presymptomatic transmission.
Household Mask Usage
It is a lot more ambiguous when it comes to household mask usage. What we do know is that wearing a mask or protective covering can reduce the emission of droplets and infectious viruses from the infectious person [17, 32, 40]. Laser light scattering studies revealed that covering the mouth of a speaker with damp cloth reduced particles emitted to background levels.
Therefore, wearing a cloth mask or even a scarf, as recommended by the Centers for Disease Control and Prevention (CDC), to cover the nose and mouth would serve to reduce respiratory emissions from an infected person, whether he is symptomatic or asymptomatic [46].
The type of mask material worn is important in mitigating the risk of infection. For instance, a study found that in a healthcare setting, the risk of influenza was substantially higher in the cloth mask group than the medical mask group [47]. Hence currently, surgical face masks and N95 respirators are still the best option, if available, for protecting a healthy person in a high-risk environment [35]. A more comprehensive experimental investigation on the protective effect of reusable cloth masks is urgently required, particularly during an extended pandemic period when a sustainable low-cost option is essential for household usage.
Studies on the effect of wearing face masks in households have been plagued by confounding factors and adherence issues. While face masks and hand hygiene have been known to be key protective measures against droplet and fomite transmission, a study of 259 households in Hong Kong showed no significant difference in the infection risk for the group that both wore face masks and observed hand hygiene [48].
A similar conclusion was reached among young adults living in university residence halls, where a combination of face masks and hand hygiene did not correlate with a significant decrease in the rate of influenza-like illness [49]. A separate study provided some insight into the underlying reason. While there was no significant decrease in infection risk by wearing face masks, it was found by self-reporting that less than 50% of study participants wore masks most of the time.
In the group that wore masks most of the time, it was found that the risk of infection decreased, with a risk ratio of 0.26, with a 95% confidence interval of 0.06 to 0.77 [50]. Face mask-wearing in households seems to be ineffective for seasonal infectious diseases. Whether or not mask-wearing at home should be regulated or recommended is doubtful, since household members will necessarily eat together, an activity during which masking is impossible. Normalcy at home is critical to mental health in a pandemic.
Public Policy and Population-Level Effects
As discussed, asymptomatic and presymptomatic cases have made pandemic containment increasingly challenging, resulting in a paradigm shift in government approaches. Undocumented cases, many of whom were asymptomatic or mildly symptomatic, were possibly contributing to a large number of infections (79%) in China [51].
A random sampling of 3000 New York residents at various locations, such as grocery stores, revealed an infection rate of 13.9%, and an estimated 2.7 million people might have been infected [52]. On 6th April, an interim guideline from the WHO stated that healthy people did not need to wear masks because there was no evidence that masks can protect the wearers [53]. This contrasted with CDC guidelines on 3rd April, which recommended cloth face coverings in public spaces, especially where there is significant community-based transmission [46].
Anecdotal evidence within hospital settings showed that universal mask usage must be implemented in high-risk areas. Symptoms of COVID-19 are similar to other respiratory diseases, and some healthcare workers displaying mild symptoms continue to work [39]. In another multiyear single-center study, a mask-wearing policy was instituted for all who interacted with hematopoietic stem cell transplant patients. Comparing the mask and premask years, respiratory viral infections decreased significantly after the mask policy. Hospital-wide and in an adjacent hematologic malignancy unit, the absence of mask policy meant that infections remained high [54].
A 2003 SARS study on five Hong Kong hospitals revealed that staff who adopted all four measures of masks, gloves, gowns, and handwashing remained healthy. Staff who omitted at least one of these practices became infected but the wearing of masks was the most significant and important measure [35]. The other three measures conferred no additional significant protection to mask wearers. Hence, stopping droplet transmission at the face level is critical.
Mathematical modelling on the 2009 (H1N1) influenza concluded that if masks were enforced early at 100 versus 1000 infectious people, the severity of an outbreak could be reduced markedly [55]. Everyone, not only infectious individuals, must wear masks to significantly reduce the cumulative number of cases. In this model, the effectiveness of surgical masks was low and insignificant. For N95 respirators operating at 20% effectiveness, a significant reduction of influenza (20%) was achieved if only 10% of the population wore them. If 25% and 50% of the population complied, the reduction became 30% and 36%, respectively.
For COVID-19, similar conclusions were achieved in a theoretical model and empirical data set study [56]. Monte Carlo simulation and an SEIR (susceptible-exposed-infectious-recovered) model were used. When a minimum of 80% of people wore masks, the impact on the pandemic was significant and the curve flattened. However, this intervention failed when 50% or less of the population wore masks.
By day 50 of a regional outbreak at the latest, universal masking could prevent widespread transmission. If enforced at day 75 with a 90% masking adoption, there was no impact on the spread of infection, highlighting the importance of early masking intervention. If at least 80% of the population wore masks, the curve could flatten more significantly than enforcing a strict lockdown. In addition, after lockdown, allowing social distancing without masking led to uncontrollable rise in infections.
With the results of these two simulations in mind, the authors studied the impact of masking enforcement on infection growth across many countries [56]. Countries can be classified into three tiers from best- to worst-performing. Across the tiers, the average daily infection growth rate and reduction from the peak are as follows: top at 5.9% and 74.6%, middle at 14.2% and 45.8%, and low at 17.2% and 37.4%.
Best-performing countries instituted universal masking orders before 15th March while those in the middle tier did this after the date. The remaining countries were the worst-performing. Overall in every region, employing universal masking resulted in better management of COVID-19.
Even though the Hong Kong government recommended mask usage only for symptomatic people, as with WHO guidelines, the general public volunteered to wear mask proactively [24]. Universal masking was also advocated by leading experts in clinical microbiology and infectious disease specialties.
After 100 days, the number of infected per million population in Hong Kong was significantly lower than countries without universal masking. The comparison was done for countries with similar population density, healthcare system, BCG vaccination, and social distancing measures.
These countries include Singapore, South Korea, Spain, Italy, and Germany. While infections and deaths have skyrocketed worldwide, Hong Kong has recorded low numbers, particularly remarkable given its close proximity to China and high population density.
The main difference causing the favourable outcome in Hong Kong was the voluntary universal masking among residents since early in the pandemic. By observation of morning commute over three consecutive days, only 3.4% out of 10,050 persons failed to wear masks.
There were eleven COVID-19 clusters which could be attributed to recreational mask-off settings such as dining and drinking in restaurants or bars, singing at karaoke parlours, and exercising in gymnasiums.
Therefore, these experiments and population studies show that universal masking is effective if implemented early and rigorously. Governments should deploy resources to obtain sufficient masks in order to achieve sustainable universal masking. If supplies are insufficient, the general public should use cloth masks when they are outside their homes. Medical masks should be reserved for healthcare workers
Understanding Performance of Commercial Mask
3-Ply Surgical Mask
The 3-ply surgical mask is commonly used in the COVID-19 pandemic. The 3-ply surgical mask is made up of 3 different layers of nonwoven fabric with each layer having a specific function, as shown in Figure 3.
- The outermost layer (typically blue) is waterproof and helps to repel fluids such as mucosalivary droplets.
- The middle piece is the filter, which prevents particles or pathogens above a certain size from penetrating in either direction.
- The innermost layer is made of absorbent materials to trap mucosalivary droplets from the user. This layer also absorbs the moisture from exhaled air, thus improving comfort.
- Together, these 3 layers effectively protect both the user and the surrounding people by limiting the penetration of particles and pathogens in both directions.

As suggested by its name, nonwoven fabric does not contain intertwining strands and is made by bonding a mass of fibres together using heat, chemical, or mechanical means. Felt is one of the most common examples of nonwoven fabric. Although nonwoven fabric is mechanically weaker than its counterpart, it is cheap and fast to manufacture. Therefore, it is an ideal material for the surgical mask. The two most common methods of making nonwoven fabric for surgical mask are spunbond and melt-blown.
The spunbond process combines the spinning and sheet formation process into one continuous, nonwoven manufacturing system [57, 58]. As seen in Figure 4, the spunbond process consists of several integrated steps, namely, extruder, gear pump, spinpack, quencher, collector, bonder, and winder.
- Extrusion is the process where the polymer is melted by heat and mechanical action of the screw
- The gear pump plays a critical role in controlling the precise volumetric flow rate of the molten polymer. This is a key step to maintain a uniform temperature of the molten polymer
- The spinpack is a die block assembly which turns the molten polymer into uniform thin filaments and is designed to be able to withstand 300°C to 400°C
- The filaments are then quenched by cool air
- After quenching, the filaments are collected together as filament web on a moving belt
- The filaments in the web are then bonded together via heat, chemical, or mechanical means to form the nonwoven fabric
- Lastly, the nonwoven fabric is collected in the winder

Schematic illustration of spunbond and melt-blown process. Republished with permission from Ref. [59]. Copyright 2015, Butterworth-Heinemann.
Although the melt-blown process is very similar to the spunbond as seen in Figure 4, the microfibres produced in melt-blown are much finer and the pore size of the nonwoven fabric can be much smaller. Therefore, due to the finer pore size, melt-blowing is the typical process used to fabricate the middle filtering piece of the 3-ply surgical mask.
The melt-blown process also consists of several integrated steps, namely, extrusion, gear pump, die assembly, collector, and winder [60]. The major difference between spunbond and melt-blown is in the die process which is the most important element responsible for the smaller diameter microfibres.
There are three components in the die assembly: the feed distribution plate, die nosepiece, and air manifold which are all kept heated at 215°C to 340°C.
- The feed distribution plate ensures the molten polymer flows across the plate evenly. The shape of the feed distribution plays an important role in the polymer distribution. The most common, coat hanger-type, has a manifold at the polymer entrance to ensure even and uniform distribution of polymer flow
- The die nosepiece is the key component which ensures the filament diameter and quality. The die tip is a very wide and thin metal piece with orifice measuring about 0.4 mm. As a result, the die tip is very fragile and has to be replaced frequently once the metal between the orifices is broken
- The air manifold, shown in Figure 5, supplies hot, high-velocity air which draws the polymer filaments into much thinner microfibres. The manifolds are unusually located at the side of the die nosepiece, and the hot air comes in contact with the polymer as it exits the die tip. The air is hot than the polymer to ensure the polymer remains liquefied during the process

Schematic illustration of air manifold in melt-blown process. Republished with permission from Ref. [61]. Copyright 2014, Woodhead Publishing Limited.
Both the spunbond and melt-blown technologies are capable of processing a great variety of thermoplastic like polypropylene, polyester, polyethylene, polyamide, and polyurethane [57, 58, 60]. Of all materials, polypropylene is the most common as it is relatively cheap and has low melt viscosity for easy processing. Coincidentally, polypropylene is the most common material used for a 3-ply surgical mask while other materials like polystyrene, polycarbonate, polyethylene, and polyester can also be used in masks [62].
….
Masks Made from Household Materials
The surge in demand worldwide for commercial face masks during the COVID-19 pandemic has led to a global shortage of supplies for both physical products as well as raw materials [80]. In this circumstance, making a mask at home can be a life-guarding action [81].
Homemade masks may vary from the commercial ones in terms of structural integrity and effectiveness, but they are cheap and accessible. Wearing a simple cloth mask is far better than wearing no mask to safeguard the wearer and the others’ health [81, 82].
Using commonly available household materials, it is easy to fabricate simple masks that may block respiratory droplets from the wearer. A lot of household materials have been used to fabricate masks and tested accordingly. These typically include cotton fabrics, clothing, silk, tissue paper, kitchen towels, pillowcase, and tea cloths.
In the H1N1 influenza pandemic, researchers tested the efficiency of homemade masks against that of commercial masks. van der Sande et al. designed a series of experiments, including short-term (10–15 mins) inward protection, long-term (3 hrs) inward protection, and outward transmission prevention, to compare the effectiveness of three types of masks under different movement activities [14].
An N95-equivalent Filtering Facepiece against Particles- (FFP-) 2 mask (1872V®, 3M), a surgical mask (1818 Tir-On®, 3M), and a homemade mask made of TD Cerise Multi® tea cloths (Blokker) were chosen. In the short-term protection test, all masks gave some protection to both adults and children against airborne particles. FFP-2 provided the best protection to adults (25 times as much as a surgical mask and 50 times as much as a homemade mask from tea cloths), while the homemade mask provided the least protection.
The protection to children was less efficient with all masks, though the efficiency ranks were the same as in adults. Activity (nodding, shaking, reading, and walking) had no obvious impact on efficiency. In the long-term protection test, the conferred protection remained highest with the FFP-2 mask and lowest with the homemade mask.
Interestingly, the measured median protection factors increased with the wearing time for the homemade mask, while they decreased with the FFP-2. In the outward protection test, the mask type significantly determined the protection factors. The homemade mask only provided marginal outward protection, while the FFP-2 and the surgical mask, which performed similarly, provided better outward protection.
Despite the relatively low effectiveness, it was suggested that wearing a homemade mask might sufficiently reduce viral exposure [12]. The marginal respiratory protection was also observed with masks made with other common materials including sweatshirts, T-shirts, towels, and scarves, when tested against polydispersed and monodispersed aerosols (20–1000 nm) [83]. Compared with the control N95 respirator, these fabric materials allowed higher penetration by aerosols, indicating poorer protection for wearers.
In addition to material, other factors, including the design, the velocity, the fitness to the wearer’s face (sealing issue), and the properties of the particles to which it will be exposed, also affect the overall performance of a homemade mask. A more comprehensive study was conducted by Davies et al., to test the efficacy of homemade masks against bacterial and viral aerosols (Bacillus atrophaeus (B. atrophaeus) with a size of 0.95–1.25 μm, and bacteriophage MS2 with a size of 0.023 μm) [12].
The masks were made from different common household materials, including 100% cotton T-shirt, scarf, tea towel, pillowcase, antimicrobial pillowcase, vacuum cleaner bag, cotton mix, linen, and silk. As shown in Table 2, all materials are capable of blocking the microorganisms to different degrees, and they all worked better in the case of B. atrophaeus due to its large size. Although the surgical mask as a control sample possesses the highest efficacy, the vacuum cleaner bag, tea towel, and cotton mix also showed filtration efficiency of higher than 70%.
The ones with the lowest efficiency were the scarf, pillowcase, and silk, most of which however still had >50% efficacy. Another important factor that needs to be considered when using a face mask is the ease of breathing, which is indicated by pressure drop. The higher the pressure drop, the higher the difficulty for the wearer to breathe.
It is obvious that despite the high filtration efficiency of a vacuum cleaner bag and tea towel, their high-pressure drop values make them unsuitable for masks. Combining the above two factors, it was suggested that the most suitable household materials for a homemade mask are pillowcase and 100% cotton t-shirt, and further studies showed that doubling the layer did not help improve the efficacy significantly [12].
Yet, doubling increased the pressure drop, indicating more difficulty for breathing. This work again provides the insight that homemade masks are capable of blocking bacteria and viruses to some extent, yet their overall performance (filtration efficiency, pressure drop, and fitness) is not comparable to N95 and surgical masks.
Indeed, wearing a mask can reduce the infection probability yet cannot eliminate the disease. It must be implemented community-wide [18] and together with multiple nonpharmaceutical preventative measures, such as hand hygiene, social distancing, quarantine, and immunization, to minimize the transmission and stop the outbreak [84]. In that sense, the homemade masks may be the last resort when facing a supply shortage, and they may well protect the general public.
Table 2
The filtration efficiency and pressure drop across materials with two different microorganisms. Reproduced with permission from Ref. [12]. Copyright 2013, Cambridge University Press.
| Material | B. atrophaeus | Bacteriophage MS2 | Pressure drop across fabric | |||
|---|---|---|---|---|---|---|
| Mean % filtration efficiency | SD | Mean % filtration efficiency | SD | Mean | SD | |
| 100% cotton T-Shirt | 69.42 (70.66) | 10.53 (6.83) | 50.85 | 16.81 | 4.29 (5.13) | 0.07 (0.57) |
| Scarf | 62.30 | 4.44 | 48.87 | 19.77 | 4.36 | 0.19 |
| Tea towel | 83.24 (96.71) | 7.81 (8.73) | 72.46 | 22.60 | 7.23 (12.10) | 0.96 (0.17) |
| Pillowcase | 61.28 (62.38) | 4.91 (8.73) | 57.13 | 10.55 | 3.88 (5.50) | 0.03 (0.26) |
| Antimicrobial pillowcase | 65.62 | 7.64 | 68.90 | 7.44 | 6.11 | 0.35 |
| Surgical mask | 96.35 | 0.68 | 89.52 | 2.65 | 5.23 | 0.15 |
| Vacuum cleaner bag | 94.35 | 0.74 | 85.95 | 1.55 | 10.18 | 0.32 |
| Cotton mix | 74.60 | 11.17 | 70.24 | 0.08 | 6.18 | 0.48 |
| Linen | 60.00 | 11.18 | 61.67 | 2.41 | 4.50 | 0.19 |
| Silk | 58.00 | 2.75 | 54.32 | 29.49 | 4.57 | 0.31 |
Historically, cloth masks have been used to protect healthcare workers (HCWs) from respiratory infections [85–87], yet it is only in recent years that researchers started to systematically study their efficacy. Chughtai et al. reviewed the use of cloth masks [88] and conducted a series of studies including randomized clinical trial (RCT) to evaluate how good the cloth masks are to protect HCWs [47, 89].
Finding that the rate of respiratory infection was highest in the cloth mask group and that the particle penetration of cloth masks was 97% (versus 44% for medical masks), the authors concluded that cloth masks should not be recommended for HCWs, especially in highly infectious situations.
Shakya et al. examined the efficiency of a cloth mask against monodispersed polystyrene latex (PSL) particles (30 nm to 2.5 μm) and diluted whole diesel exhaust [90]. It was found that with an exhaust valve, the cloth mask had a filtration efficiency of 80-90% against PSL particles. Without a valve, the efficiency against the same PSL particles drops to 36-65%, although the cloth mask performed better against larger particles.
The cloth mask’s filtration efficiency ranged from 15 to 75% against whole diesel particles. The overall performance results suggested that cloth masks provided marginal protection to the wearer from particles less than 2.5 μm. Furthering the study on filtration efficiency, Neupane et al. investigated the effect of washing and drying of cloth masks on the filtration performance and correlated the performance to the pore size and shape in the masks [91].
It was found that the PM10 filtration efficiency dropped by 20% after the 4th washing and drying cycle, which was ascribed to the increase in pore size and the lack of microfibres within the pore region. Long-term usage of the cloth masks entails continuous stretching of the mask, enlarging the pore size, thus impairing mask performance.
Making a cloth mask can be as simple as combining two cloth layers with stretchable ear loops (Figure 8(a)) [91]. Sugrue et al. introduced a step-by-step method of making a cloth mask using household materials including cotton, metal garden wire, and elastic bands (Figure 8(b)) [92].
The fabricated cloth mask has demonstrated its good comfort and fitness to the human face. While one can also find instructions on how to sew a fabric face mask at home [93, 94], Konda et al. recently developed a new model to fabricate homemade cloth masks that can achieve high filtration efficiency against aerosol particles ranging from 10 nm to 10 μm in size [95].
By combining different commonly available fabrics, for instance, cotton-silk, cotton-chiffon, cotton-flannel, and filtration efficiency for particles < 300 nm and >300 nm can be as high as >80% and >90 %, respectively. The high efficiency comes from the synergistic effect of mechanical filtration from cotton and electrostatic filtration from the other layer like silk (Figure 9).
It was also highlighted in this work that for the same material such as cotton, there are other factors that critically and significantly affect the overall performance when used as a mask. These include the layer number, the layer density (threads per inch, TPI), and the facial fitness (openings and gaps between the mask edge and the facial contours). Therefore, future mask development should consider the above factors while taking into consideration the breathability, washability, and reusability.

(a) Photos showing examples of simple cloth masks. Reproduced with permission from Ref. [91]. Copyright 2019, Neupane et al., PeerJ. (b) Schematic showing the pattern for a homemade mask. Reproduced with permission from Ref. [92]. Copyright 2020, Springer Nature.

A new design of homemade cloth masks from common fabric materials. Reproduced with permission from Ref. [95]. Copyright 2020, the American Chemical Society.
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7429109/
More information: Shubham Sharma et al, On secondary atomization and blockage of surrogate cough droplets in single- and multilayer face masks, Science Advances (2021). DOI: 10.1126/sciadv.abf0452



{kind=link}
[…] COVID-19: Why are three layer masks safer than one or two… […]