











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



As the COVID-19 pandemic has progressed, it has become clear that many survivors – even those who had mild cases -continue to manage a variety of health problems long after the initial infection should have resolved.
In what is believed to be the largest comprehensive study of long COVID-19 to date, researchers at Washington University School of Medicine in St. Louis showed that COVID-19 survivors – including those not sick enough to be hospitalized – have an increased risk of death in the six months following diagnosis with the virus.
The researchers also have catalogued the numerous diseases associated with COVID-19, providing a big-picture overview of the long-term complications of COVID-19 and revealing the massive burden this disease is likely to place on the world’s population in the coming years.
The study, involving more than 87,000 COVID-19 patients and nearly 5 million control patients in a federal database, appears online April 22 in the journal Nature.
“Our study demonstrates that up to six months after diagnosis, the risk of death following even a mild case of COVID-19 is not trivial and increases with disease severity,” said senior author Ziyad Al-Aly, MD, an assistant professor of medicine. “It is not an exaggeration to say that long COVID-19 – the long-term health consequences of COVID-19 – is America’s next big health crisis.
Given that more than 30 million Americans have been infected with this virus, and given that the burden of long COVID-19 is substantial, the lingering effects of this disease will reverberate for many years and even decades. Physicians must be vigilant in evaluating people who have had COVID-19. These patients will need integrated, multidisciplinary care.”
In the new study, the researchers were able to calculate the potential scale of the problems first glimpsed from anecdotal accounts and smaller studies that hinted at the wide-ranging side effects of surviving COVID-19, from breathing problems and irregular heart rhythms to mental health issues and hair loss.
“This study differs from others that have looked at long COVID-19 because, rather than focusing on just the neurologic or cardiovascular complications, for example, we took a broad view and used the vast databases of the Veterans Health Administration (VHA) to comprehensively catalog all diseases that may be attributable to COVID-19,” said Al-Aly, also director of the Clinical Epidemiology Center and chief of the Research and Education Service at the Veterans Affairs St. Louis Health Care System.
The investigators showed that, after surviving the initial infection (beyond the first 30 days of illness), COVID-19 survivors had an almost 60% increased risk of death over the following six months compared with the general population.
At the six-month mark, excess deaths among all COVID-19 survivors were estimated at eight people per 1,000 patients. Among patients who were ill enough to be hospitalized with COVID-19 and who survived beyond the first 30 days of illness, there were 29 excess deaths per 1,000 patients over the following six months.
“These later deaths due to long-term complications of the infection are not necessarily recorded as deaths due to COVID-19,” Al-Aly said. “As far as total pandemic death toll, these numbers suggest that the deaths we’re counting due to the immediate viral infection are only the tip of the iceberg.”
The researchers analyzed data from the national health-care databases of the U.S. Department of Veterans Affairs. The dataset included 73,435 VHA patients with confirmed COVID-19 but who were not hospitalized and, for comparison, almost 5 million VHA patients who did not have a COVID-19 diagnosis and were not hospitalized during this time frame.
The veterans in the study were primarily men (almost 88%), but the large sample size meant that the study still included 8,880 women with confirmed cases.
To help understand the long-term effects of more severe COVID-19, the researchers harnessed VHA data to conduct a separate analysis of 13,654 patients hospitalized with COVID-19 compared with 13,997 patients hospitalized with seasonal flu. All patients survived at least 30 days after hospital admission, and the analysis included six months of follow-up data.
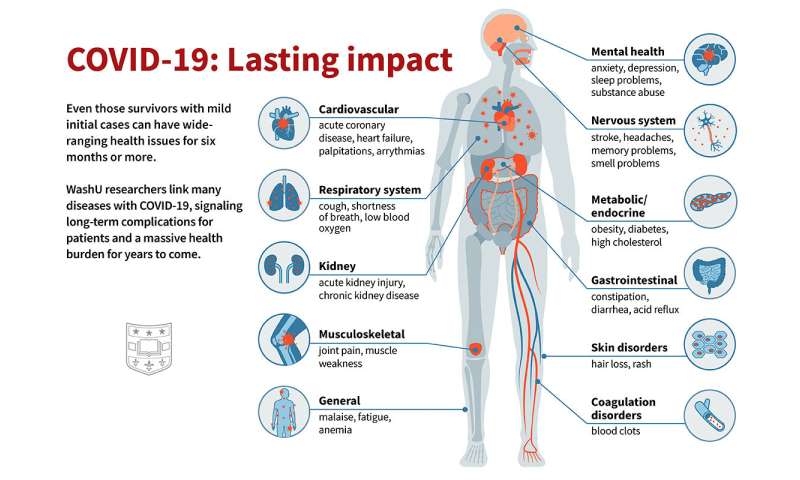
The researchers confirmed that, despite being initially a respiratory virus, long COVID-19 can affect nearly every organ system in the body. Evaluating 379 diagnoses of diseases possibly related to COVID-19, 380 classes of medications prescribed and 62 laboratory tests administered, the researchers identified newly diagnosed major health issues that persisted in COVID-19 patients over at least six months and that affected nearly every organ and regulatory system in the body, including:
- Respiratory system: persistent cough, shortness of breath and low oxygen levels in the blood.
- Nervous system: stroke, headaches, memory problems and problems with senses of taste and smell.
- Mental health: anxiety, depression, sleep problems and substance abuse.
- Metabolism: new onset of diabetes, obesity and high cholesterol.
- Cardiovascular system: acute coronary disease, heart failure, heart palpitations and irregular heart rhythms.
- Gastrointestinal system: constipation, diarrhea and acid reflux.
- Kidney: acute kidney injury and chronic kidney disease that can, in severe cases, require dialysis.
- Coagulation regulation: blood clots in the legs and lungs.
- Skin: rash and hair loss.
- Musculoskeletal system: joint pain and muscle weakness.
- General health: malaise, fatigue and anemia.
While no survivor suffered from all of these problems, many developed a cluster of several issues that have a significant impact on health and quality of life.
Among hospitalized patients, those who had COVID-19 fared considerably worse than those who had influenza, according to the analysis. COVID-19 survivors had a 50% increased risk of death compared with flu survivors, with about 29 excess deaths per 1,000 patients at six months. Survivors of COVID-19 also had a substantially higher risk of long-term medical problems.
“Compared with flu, COVID-19 showed remarkably higher burden of disease, both in the magnitude of risk and the breadth of organ system involvement,” Al-Aly said. “Long COVID-19 is more than a typical postviral syndrome. The size of the risk of disease and death and the extent of organ system involvement is far higher than what we see with other respiratory viruses, such as influenza.”
In addition, the researchers found that the health risks from surviving COVID-19 increased with the severity of disease, with hospitalized patients who required intensive care being at highest risk of long COVID-19 complications and death.
“Some of these problems may improve with time—for example, shortness of breath and cough may get better—and some problems may get worse,” Al-Aly added.
“We will continue following these patients to help us understand the ongoing impacts of the virus beyond the first six months after infection. We’re only a little over a year into this pandemic, so there may be consequences of long COVID-19 that are not yet visible.”
In future analyses of these same datasets, Al-Aly and his colleagues also plan to look at whether patients fared differently based on age, race and gender to gain a deeper understanding of the risk of death in people with long COVID-19.
As of Jan 4, 2021, the global pandemic of COVID-19—an emerging infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)—has resulted in more than 83 million confirmed cases with more than 1·8 million deaths. The epidemiological and clinical characteristics, pathogenesis, and complications of patients with COVID-19 at acute phase have been explicitly described,1, 2 but the long-term consequences of the illness remain largely unclear.
Long-term follow-up studies on persistent symptoms, lung function, physical, and psychological problems of discharged patients are urgently required.3 Only a few studies with limited sample size have been published, with the longest follow-up duration of 3 months following discharge from hospital.4, 5, 6, 7, 8
Some persisting symptoms such as fatigue and dyspnoea,4, 8 impaired pulmonary function,5, 7 and chest image abnormalities6 were reported in patients following hospital discharge, but the full spectrum of post-discharge characteristics is still unknown.
Furthermore, no studies have yet reported the extra-pulmonary organ manifestations that could persist after damage in acute stage or are new onset after discharge.
We aimed to describe the long-term consequences of COVID-19 in patients after hospital discharge and identify the potential risk factors, including disease severity, associated with these consequences.
Discussion
To our knowledge, this is the largest cohort study with the longest follow-up duration assessing the health consequences of adult patients discharged from hospital recovering from COVID-19. We found that at 6 months after symptom onset, most patients endorsed at least one symptom, particularly fatigue or muscle weakness, sleep difficulties, and anxiety or depression. More severely ill patients had increased risk of pulmonary diffusion abnormality, fatigue or muscle weakness, and anxiety or depression. The seropositivity and titres of the neutralising antibodies were significantly lower than at acute phase.
We found that fatigue or muscle weakness, sleep difficulties, and anxiety or depression were common, even at 6 months after symptom onset. This is consistent with data from previous SARS long term follow-up studies. Canadian researchers found that most SARS survivors had good physical recovery from their illness, but 33% reported a significant decrement in mental health 1 year later.23
A follow-up study of SARS survivors showed that 40% of patients still had a chronic fatigue problem for a mean period of 41·3 months after SARS.24 We found that being a woman and severity of illness were risk factors for persistent psychological symptoms. Female SARS survivors had higher stress levels and higher levels of depression and anxiety.25 In a 3-month follow-up survey of 538 COVID-19 patients, Xiong and colleagues8 found that physical decline or fatigue, post-activity polypnoea, and alopecia were more common in women than in men.
The underlying mechanism of the psychiatric consequences of COVID-19 is likely to be multifactorial and might include the direct effects of viral infection, the immunological response, corticosteroid therapy, ICU stay, social isolation, and stigma.26
The results of lung function assessment in this study showed that a considerable proportion (22–56% across different severity scales) of participants had a pulmonary diffusion abnormality 6 months after symptom onset. This was consistent with findings that the most common abnormal CT pattern was pulmonary interstitial change (GGOs and irregular lines), which were similar to the long-term lung manifestations of SARS27 or influenza.28 Respiratory viral infection might potentially induce distinct fibroblast activation in the convalescence phase.29
The disease severity in the acute phase was found to be associated with pulmonary diffusion abnormality and percentage change of CT score in the multivariable analysis. Our results did not suggest that corticosteroids could accelerate the recovery of lung injury on pulmonary function assessment and chest imaging, although evidence has shown the benefits of corticosteroid treatment for patients with COVID-19.30, 31 Whether the remaining radiological or pulmonary diffusion abnormalities completely resolve needs to be investigated in further follow-up studies.
In this study, we found that the seropositivity and median titres of the neutralising antibodies were significantly lower compared with at acute phase. In a report assessing 30 082 patients with mild-to-moderate COVID-19, although antibody titres were stable over a period of 3 months, a modest decline was observed at the 5-month timepoint.32 Among asymptomatic individuals, 81% had reduction of neutralising antibody concentrations during the early convalescent phase.33 The decline of neutralising antibodies observed in the present study and other studies raises concern for SARS-CoV-2 re-infection. The risk of re-infection should be monitored for patients who present with compatible symptoms of COVID-19.
Our study also investigated long-term extrapulmonary organ manifestations and death during follow-up. For example, persistent renal dysfunctions were observed, some participants were newly diagnosed with diabetes, and venous thromboembolic diseases, (including cardiovascular and cerebrovascular events) occurred. Angiotensin-converting enzyme 2—enriched in the renal proximal tubule34, 35—could mediate the entry of SARS-CoV-2 into epithelial cells to accumulate and cause cytotoxicity and inflammatory cell infiltration.
A previous study reported that persistent impairment in renal function can occur following an episode of acute kidney injury, with the potential to progress to end-stage kidney disease with dialysis.36 The limitation of serum creatinine to diagnose acute kidney injury has been underscored, which might result in underestimation of patients with acute kidney injury at acute phase.37 For the first time, we showed that 13% of patients without acute kidney injury and with normal eGFR at the acute phase had decreased eGFR at follow-up.
The persistent follow-up of discharged patients with COVID-19 is necessary and essential, not only to understand the association between extrapulmonary diseases and SARS-CoV-2 infection, but also to find ways to reduce morbidity and mortality by efficient prevention.
This study has several limitations. Firstly, the baseline data of pulmonary function and 6-min walking distance are unavailable. However, the proportion of patients with chronic pulmonary and heart disease in this cohort is fairly low, although self-reported by patients which might have resulted in underestimation.
The observed impaired pulmonary function and exercise capacity cannot be directly attributed to COVID-19. Secondly, for new symptom onset after COVID-19, the data were not stratified further to determine if the symptoms were persistent following COVID-19, worsened after COVID-19 recovery, or occurred post-discharge.
Thirdly, patients with mild COVID-19 symptoms who had stayed in Fangcang shelter hospitals38 were not enrolled. Further efforts are needed to compare the long-term outcomes between inpatients and outpatients. Finally, the number of participants with SARS-CoV-2 antibody test results both at acute phase and follow-up was limited. In the future, a larger sample is needed to clarify the dynamic changes of antibodies against SARS-CoV-2.
At 6 months after symptom onset, fatigue or muscle weakness and sleep difficulties were the main symptoms of patients who had recovered from COVID-19. Risk of anxiety or depression as an important psychological complication and impaired pulmonary diffusion capacities were higher in patients with more severe illness. These results support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7833295/
More information: Al-Aly Z, Xie Y, Bowe B. High dimensional characterization of post-acute sequalae of COVID-19. Nature. April 22, 2021. DOI: 10.1038/s41586-021-03553-9



{kind=link}