











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



New research presented at this year’s European Congress on Obesity (held online, 10–13 May) reveals an association between increasing body mass index (BMI) and the risk of testing positive SARS-CoV-2, the virus which causes COVID-19.
The study is by Dr. Hadar Milloh-Raz, The Chaim Sheba Medical Center, Tel-HaShomer, Ramat-Gan, Israel, and colleagues.
Obesity-related factors, including changes to the innate and adaptive immune systems brought on by excess weight, are believed to be associated with an increased risk of contracting various viral diseases. This association between BMI and viral infection risk suggests that a similar relationship may also exist between an individual’s BMI and their risk of contracting SARS-CoV-2.
This study aimed to assess the relationship between BMI and likelihood testing positive in patients who were tested for SARS-CoV-2 at the largest medical center in the Middle East. The team analyzed the details of patients who had been tested for the virus during a 9-month period, collecting data on BMI, age, sex, and presence of comorbidities including congestive heart failure (CHF), diabetes mellitus (DM), hypertension (HTN), ischemic heart disease (IHD), stroke (CVA), and chronic kidney disease (CKD). The study did not look at COVID-19 mortality or outcomes, only the risk of testing positive.
At the start of the pandemic, the Chaim Sheba Medical Center introduced a policy in which all hospitalized patients were tested for COVID-19, regardless of their symptoms or reason for admission (whether they were suspected to have COVID-19, or for completely different reasons such as elective surgery, traffic accidents).
In total 26,030 patients were tested across the study period (between March 16 and December 31, 2020), and 1,178 positive COVID-19 results were recorded. The numbers of patients in each BMI category and the proportion of positive tests varied as shown in the table:
The authors found that the odds of testing positive for SARS-CoV-2 were significantly higher in patients who were overweight or obese compared to those with a normal BMI. Those patients classed as overweight (BMI 25.0-29.9 kg/m2) were 22% more likely to test positive than those of normal weight (BMI 18.5-24.9 kg/m2).
The likelihood of testing positive was even higher in patients with obesity relative to their normal weight counterparts, and those odds rose with increasing BMI. Class I obesity (BMI 30.0-34.9 kg/m2) was linked to a 27% higher risk of testing positive, which increased to 38% for class II obesity (BMI 35.0-39.9 kg/m2), and an 86% higher risk in class III or morbid obesity (BMI at or above 40.0 kg/m2).
The relationship between BMI and the probability of a patient testing positive remained significant even after adjusting for the age and sex of the patient and having accounted for any comorbidities that were present. The authors found that every 1 kg/m2 rise in a patient’s BMI was associated with an increase of around 2% in the risk of testing positive for SARS-CoV-2.
The study also found both positive and negative associations between the risk of testing positive and the presence of comorbidities linked to obesity. Diabetes was associated with a 30% higher likelihood of testing positive, while the risk of testing positive was almost six times greater in patients with hypertension.
Conversely, the authors found that the odds of a positive test were 39%, 55%, and 45% lower among patients with a history of stroke, IHD, and CKD, respectively. The authors cannot provide an explanation for why patients with stroke, IHD or CKD would have a lower risk of testing positive for SARS-CoV-2.
The authors conclude: “As BMI rises above normal, the likelihood of a positive SARS-CoV-2 test result increases, even when adjusted for a number of patient variables. Furthermore, some of the comorbidities associated with obesity appear to either be associated with an increased risk of infection or to be protective.”
Obesity and the metabolic link to COVID-19
Literature data state that there is a direct metabolic link between the state of inflammation (such as the one associated with diabetes and metabolic syndrome) and the ‘cytokine storm’ contributing to the respiratory decline of COVID-19 patients. The entry of the virus to the cell is mediated by the ACE2 ectoenzyme located at the cell surface in the lungs and by the serine protease TMPRSS2; thus, the correlation with the renin-angiotensin system is obvious.
Indeed, ACE1 activity is increased and ACE2 inhibited; while angiotensin II activates angiotensin receptors 1 and 2 (AT1R, AT2R) mediating a pro-inflammatory response, and a consequent increase of vascular permeability. Importantly, this metabolic imbalance is aggravated by pre-existing diabetes or hypertension, usual consequences of obesity (9,10).
Moreover, some drugs frequently used for treatment of obese patients complications (such as antihypertensives, statins, thiazolidinediones) have the tendency to up-regulate ACE2, thus increasing the viral up-take (11–13). Previous preclinical studies in an animal model showed that the association of diabetes with MERS-CoV dampened the ability of the body to engage an effective immune response and induced a poor recovery after illness (14).
The disease burden of obesity is obvious in hospitalized COVID-19 patients and has strong relationship with the development of obese-related major and lethal complications. Obesogenic comorbidities (15,16) have become major health problems in hospitalized patients including increased insulin resistance (17–20) and type 2 diabetes (21), fatty liver diseases (22,23), vascular inflammation and coronary heart disease (24,25), immune diseases (26), risk of cerebral ischemia and brain injury (27), atherosclerotic vascular disease and myocardial infarction (28) as well as cancers (29). Adipose tissue and adipocytes produce leptin and other molecules that affect the cardiovascular function. The production of these substances is perpetrated through distinct endocrine, autocrine and paracrine mechanisms and believed to lead to cytokine-mediated inflammatory changes in the liver and systemic inflammation and atherosclerosis (30–33).
Smethers and Rolls (34) reported that, in obese adults, the correlation between unhealthy eating patterns or uncontrolled eating management and immune deficiency is highly complex. Systematic reviews (35,36), research studies (37) and meta-analyses (38) have documented that high-energy diets are a risk factor for weight gain. Nutritional patterns collectively termed as ‘Western diet’, include trans- and saturated high-fats and cholesterol, high-protein, high-sugar, excess salt intake, low in complex carbohydrates, fiber, micronutrients such as vitamin D (39) and are all associated with impaired inflammatory pathways (40–47).
Frequent consumption of processed, ‘fast foods’ or foods contaminated with pesticide residues predispose individuals to inflammation through the increased uptake of lipopolysaccharide from microbes in the gut because of increased gut leakiness (48) as well as promote obesity and metabolic syndrome (15). Furthermore, unhealthy diet has been correlated to autoimmune pathology such as multiple sclerosis (49), rheumatoid arthritis (50), inflammatory bowel disease (51), systemic lupus erythematosus (52) and psoriasis, through specific deregulations of T cells (Treg) that particularly promote leptin (53) and TH17-biased immunity, partly dependent on increased IL-6 (54). Importantly, excess dietary salt intake is associated with obesity (55), hypertension, cardiovascular disease and stroke (56), through the enhancement of pathogenic TH17 cells (57) as well as p38/MAPK and nuclear factor of activated T cells 5 (NFAT5) activation (58), due to cellular response to hyperosmotic environments (59).
The pulmonary tissue is the most sensitive human tissue in intensive care unit (ICU) COVID-19 patients. Systemic hypoxia due to reduced pulmonary functions, increased adipokines and cytokines, gut (60) and pulmonary (61) microbiome alterations (62), cardiopulmonary, vascular and epithelial complications due to chronic obstructive pulmonary disease (63) are cofactors associated with critical illness among hospitalized patients with COVID-19 disease reported in Zhanjiang province (64) and Jiangsu province, China (65) as well as in New York City, USA (66). Petrilli et al pointed out that, in COVID-19 ICU patients, the highest risks are exhibited by those aged ≥75 years, body mass index (BMI) >40 and heart failure. Moreover, strong critical illness parameters were admission oxygen saturation <88%, d-dimer >2,500, ferritin >2.500 as well as C-reactive protein (CRP) >200.
Age and obesity
Aging seems to present with a great variety of patterns and unique sets of obesity and age-related disease. Among older adults, independent of their BMI, blood pressure and blood lipid concentrations (67), decline in immune function is observed (known as immune-senescence) leading to increased susceptibility and exhibiting more serious complications as compared to younger individuals; reflecting the deterioration of function in both the acquired and innate immune systems (20,45,68). In elderly, most cells produce cytokines/chemokines/adipokines and soluble mediators of inflammation due to inflammation-related gene expression by ROS induced lipid oxidation-derived products and formation of lipid droplets within the monocytes/macrophages (69).
Ageing is also associated with a multi-factorial decrease of T cell function and number, T-cell subset composition and functional capacity, fewer naive T cells, more memory cells in the circulation, thymic involution and decreased thymic output and naive T cells as well as increased memory cells in the circulation (70). Furthermore, modifications of immunoglobulin levels, micronutrient deficiencies (71) and biological dysfunctions including lymphocyte proliferation and cytokine production, thus increasing inflammation, as well as hospitalization and death have been documented (72).
In March 2020 (1) a review was published on the 2019 outbreak (COVID-19) supporting that ‘COVID-19 lethality is proving to be higher than previous epidemics on account of international travel density and immune naivety of the population’. In obese COVID-19 patients, the adipose tissue interacts with the immune system facilitating the severity and lethality of the disease through biochemical, molecular, cellular as well as immune interplay.
The World Health Organization (WHO) has characterized both the COVID-19 outbreak and obesity ‘epidemic’ as international public health emergencies. Global clinical and epidemiological observations confirm that CoVs can cause more severe symptoms and complications in people with obesity-related conditions. Indeed, Wu et al (4) established the correlation between obesity-induced immune deficiency and COVID-19 adverse outcomes.
Obesity and inflammation
Immunologically, obesity is characterized as a chronic sub-clinical inflammatory morbid entity which can impact the immune responses to infectious diseases through direct, indirect and epigenetic (73,74) mechanisms. Evans et al (75) described various fat tissue-associated cytokines (adipokines) that are produced and released in proportion to the amount of visceral adipose tissue in the body.
Serum amyloid-A is an adipokine secreted by adipocytes, that can act directly on macrophages to increase their production of inflammatory cytokines such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, and IL-6, and resistin (22,23,75). Indeed, Alam et al (76) reported in detail that the majority of respective adipokines are inflammatory mediators such as IL-8, PAI-1, MCP-1, IL-6, IL-1Ra, TNF-α, sTNFRII, and IL-18.
In addition, IL-8, IL-10, interferon gamma (IFN-γ) and inducible protein 10 (IP-10 or CXCL10) have been shown to be associated with excessive body weight (77). Obesity-induced adipokine production such as leptin /adiponectin ratio increases insulin resistance in type 2 diabetes, resulting in inability to feel and detect satiety leptin in the arcuate nucleus of mediobasal hypothalamus (78). Moreover, adverse effects are evident, despite high energy stores, on hunger, food energy use, physical exercise and energy balance as well as on hippocampus-mediated deficit in learning and memory functions (79).
Furthermore, the prolonged IFN responses during persistent chronic inflammation and obesogenesis comprise reciprocal causality between virus susceptibility and obesity (80). Additional epigenetic signatures in obesity are likewise altered including methylation and/or histone acetylation levels in genes involved in specific and general metabolic processes, altering thus, the metabolic phenotype of the offspring (81–83). Although no specific therapy exists to block the effects of these factors, recognizing the high risk and anticipating inflammation-associated complications of adipokine release is an important part of optimal patient management.
Obesity and immune response
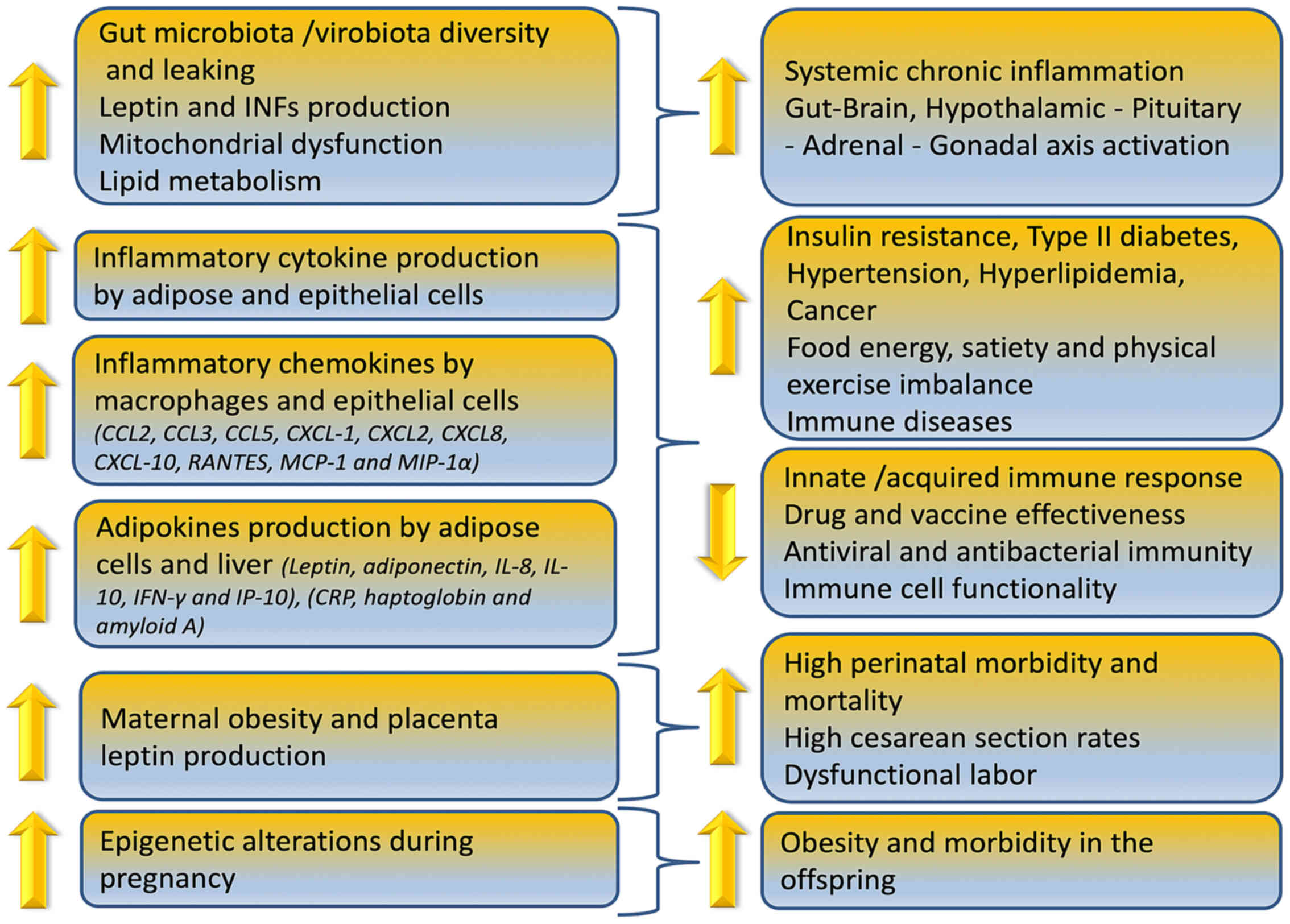
Obesity can reduce immune cell functionality, induce gut microbiome/virome imbalance, inflammatory cytokine phenotype and increase antiviral, antimicrobial and anticoagulant resistance as depicted in Fig. 1. In overweight children, anti-tetanus IgG antibodies were significantly lower compared to normal weight controls due to the chronic low grade inflammation expressed by the higher levels of IL-6 (84). Similarly, researchers reported in a 2019 study that reduction or elimination of food in overweight/obese adults can lead to a decreased IgG concentration over time (85).
The mechanisms involved in increased risk for higher COVID-19 prevalence and mortality in obese are correlated with specific fat-resident regulatory T cells (86) (Treg) and particularly promotion of TH17 (T-cell sub-lineage)-biased immunity (87,88). Indeed, these processes are partly dependent on increased IL-6, as well as IL-23/IL-17, other inflammatory obesity-associated plasma cytokine expression such as TNF-α, transforming growth factor (TGF), pro-inflammatory cytokine macrophage migration inhibitory factor and macrophage inflammatory protein-1α (89).
Furthermore, in this mechanism increased CRP levels (90) and disrupted tight junctions in pulmonary epithelia (91) have also been implicated. Additionally, Ahmed and Gaffen (92) argued that ‘obesity selectively promotes expansion of the Th17 T-cell lineage, exacerbating immune diseases in specific organs in obese individuals, such as brain and gut, according to the results of new experimental and human studies. Th17 cells are also associated with autoimmune disease such as multiple sclerosis, rheumatoid arthritis, and psoriasis (93), but also glomerulonephritis, asthma, and pandemic H1N1 influenza virus (94).
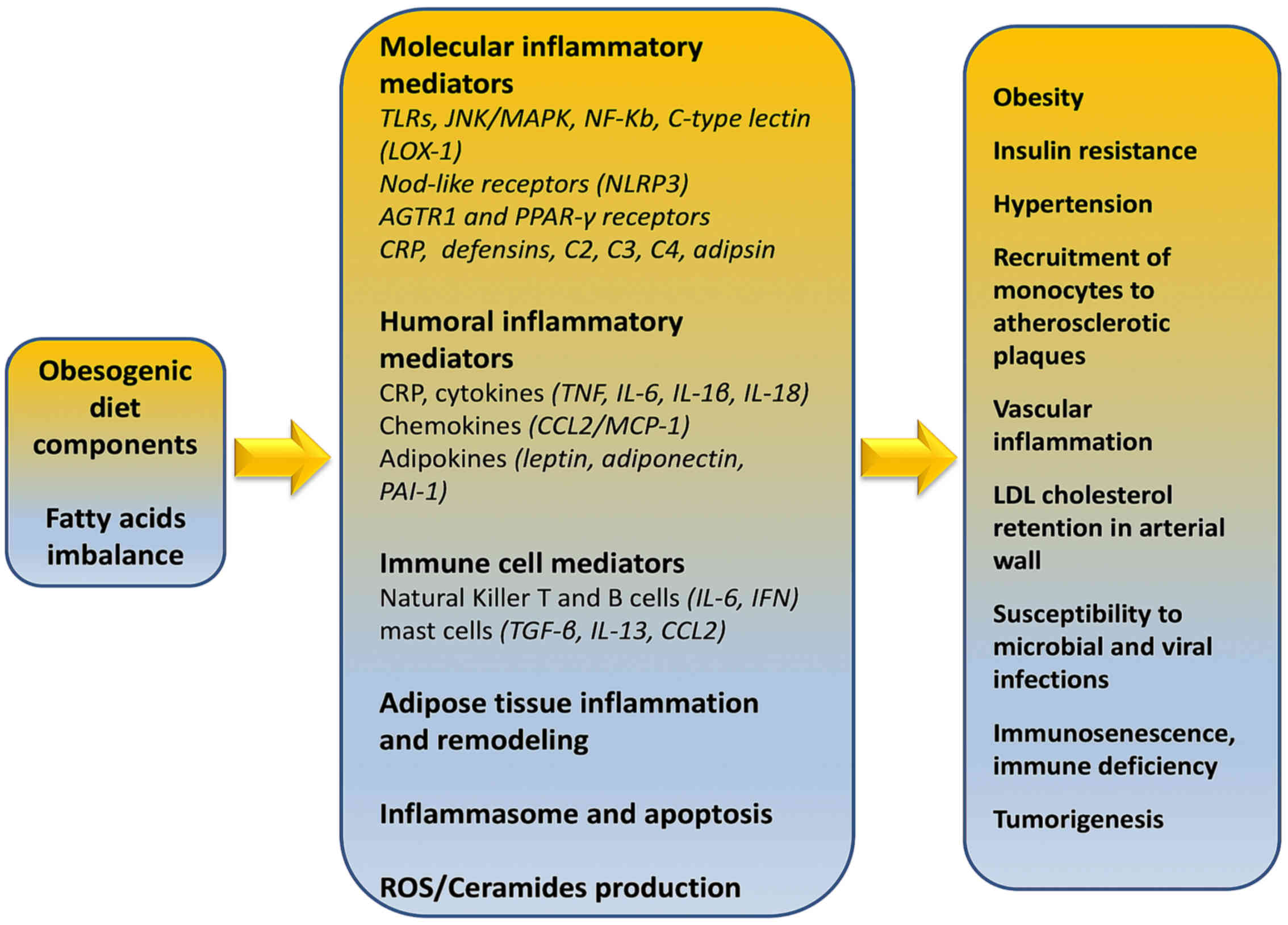
Strissel et al (95) demonstrated that adipose tissue inflammation as well as the resistance to insulin action in adipocytes are accelerated by a high fat diet. This induces the mobilization of T cells (predominantly CD4+ and CD8+) to adipose tissue and associated increased synthesis of IFNγ thus, contributing to the local inflammatory responses (Fig. 2). Inflammatory T helper cells secreting cytokines including IL-1β, IL-6, IL-8, IL-10, TNF-α, granulocyte- and macrophage-colony stimulating factor (GM-CSF) are present both in obese phenotype and COVID-19 patients, affecting prognosis, pathogenesis and fatality.
According to Zhou et al (96), COVID-19 entry into the cell leads to over-production of inflammatory cytokines. Importantly, in ICU patients infected with SARS-CoV-2, the expression of specific proteins increased significantly, suggesting an exhausted status of T cells. COVID-19 ICU patients with severe pneumonia showed correlated higher percentage of GM-CSF+ and IL-6+CD4+ T cells.
The inflammatory signature of monocytes (CD14+CD16+ with high expression of IL-6) is similar in ICU COVID-19 patients and obese adults with inflammatory phenotype. Therefore, activated immune cells may enter the pulmonary circulation in large numbers and exert a damaging role especially in obese COVID-19 patients with severe pulmonary syndrome caused by pathogenic GM-CSF+ Th1 cells and inflammatory CD14+ and CD16+ monocytes.
Indeed, a cytokine-abundant environment, aberrant pathogenic Th1 cells, inflammatory CD14+, CD16+ monocytes, the high expression of IL-6 and intense inflammatory monocytes infiltration, to pulmonary circulation, accelerate the inflammation and affect pulmonary immune-pathology leading to deleterious clinical manifestations, lung functional disability and even acute mortality.
On April 15, 2020, the Centers for Disease Control and Prevention (CDC), based on currently available information and clinical expertise, advised that older adults and people of any age who have serious underlying medical conditions, including obesity with a BMI of 40 or above, might be at higher risk for complications and severe illness from COVID-19. In this report, emphasis is given on ascertainment that severe obesity increases the risk of acute respiratory distress syndrome (ARDS) (3).
Obesity, increased food intake, nutrient/energy imbalance affect in a bidirectional way the immune deficiency, especially in vulnerable populations. Patients with type 2 diabetes and those with metabolic syndrome (pre-diabetes) may be up to ten times more likely to die when they become ill with COVID-19 (9).
The mortality rate for young people who had to be admitted to a hospital with severe respiratory illness due to COVID-19 was approximately 2%, but this increased to 14% for the most vulnerable such as COVID-19 patients with obesity and related co-morbidity (97). For autoimmune diseases, such as systemic lupus erythematosus, systemic vasculitis and rheumatoid arthritis, treatment may include drugs including methotrexate and hydroxychloroquine (Plaquenil) that suppress the immune system to treat the disease and symptoms making immune-compromised patients more vulnerable to COVID-19 infection (98).
Foods may have calories, but do not contain vitamins, minerals, antioxidants etc., indicating that increased calorie intake, in relation to nutrient intake, is the main reason behind the immunodeficiency today. For example, even short-term severe vitamin D deficiency (99) may directly promote hypertension and impacts on renin-angiotensin system components that could contribute to target-organ damage (100). Nutrient deficiencies are highly prevalent in the United States (and elsewhere), increasing much of the consequent risk of premature aging, chronic disease and COVID-19 prevalence and mortality due to acceleration of the risk associated with aging (101).
In addition low dietary antioxidant intake (102), occupational exposures (103) and increased genetically modified foods (104) including cotton seed/canola seed/corn oil, eggplant, fruits and vegetables e.g., papaya, potatoes, tomatoes, lettuce may enhance immune system deficiency (105).
Lipotoxicity and obesity
Lipotoxicity is a condition, induced by the aggregation of intermediate lipids to non-fatty tissue, which leads to cell malfunction and death (106). Tissues that are usually affected include kidneys, liver, heart, and skeletal muscle. Lipotoxicity is believed to play a role in heart failure, obesity and diabetes and is estimated to affect approximately 25% of the adult American population (20,45,107,108).
Under physiological conditions, there is a balance between cellular lipid production and their oxidation or transport. However, this balance might be disrupted when the cells are lipotoxic, that is, when an imbalance between the amount of cellular lipids produced and the amount consumed is evident. Thus, upon fatty acids entry to cells, conversion to various types of storage lipids is initiated. Triacylglycerol (TG), consisting of a glycerin molecule bound to three fatty acids, is established as the safest type of intracellular lipid storage. Apart from TG, fatty acids can be converted to fatty acyl-CoAs, ceramides and diacylglycerol. Importantly, these molecules were shown to induce lipotoxicity when found in high concentrations and can inflict damage to cells (109).
It is not well-established whether lipotoxicity is related to genetic or non-genetic causes, but it is not considered to be a single-gene disease. Opinions which argue that obesity can either attenuate or facilitate lipotoxicity exist. Indisputably, a high-fat diet increases the risk for this pathological condition. Importantly, individuals with high number of lipotoxic cells appear to be resistant to both insulin and leptin (110).
Oxidative stress, reactive oxygen species, lipid peroxidation
Initially the term oxidative stress was defined as the imbalance between pro-oxidants and antioxidants in favor of the former (111). Over the years, this definition is based on new data, and oxidative stress is now considered a disorder of the redox signaling (112).
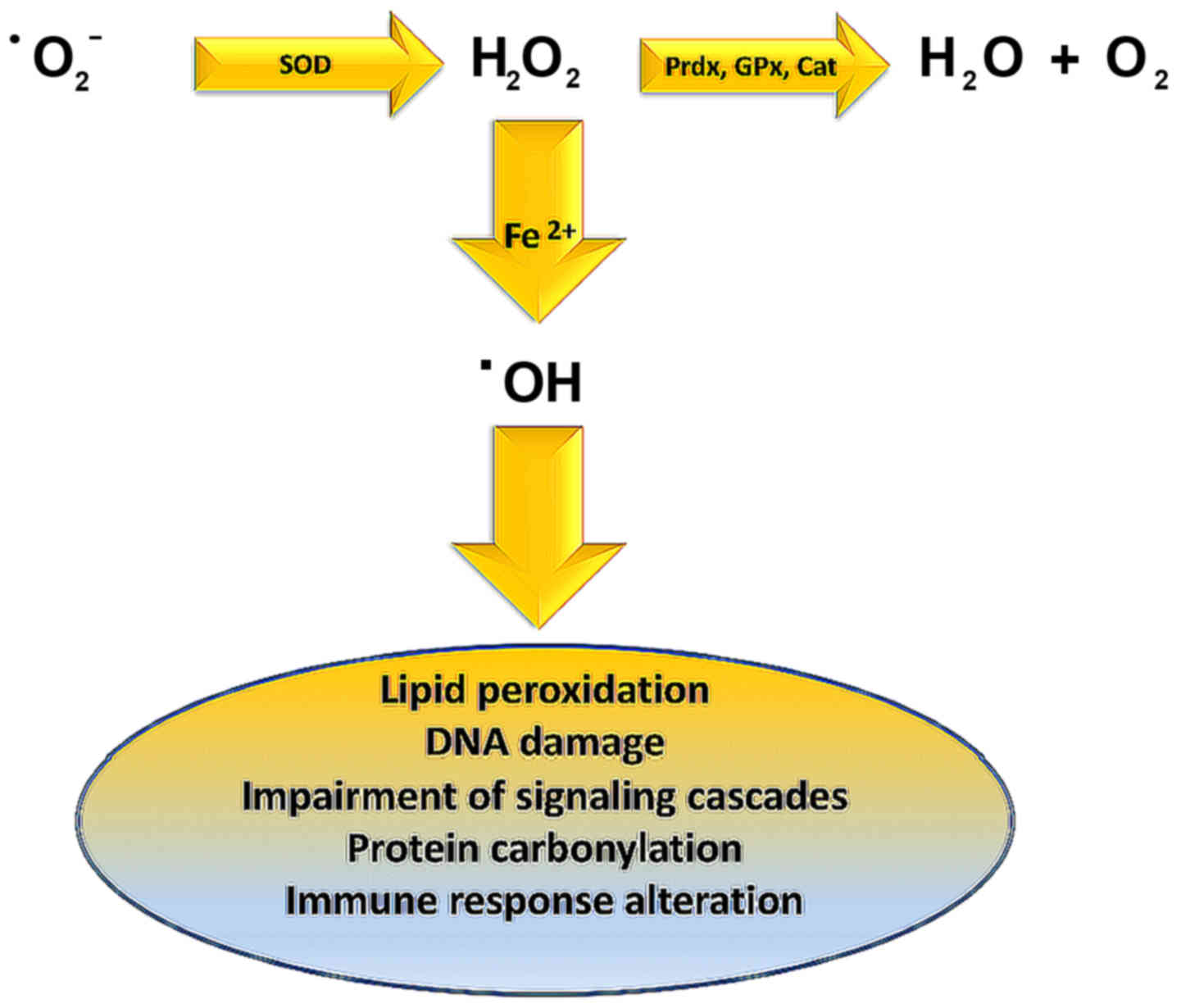
Lipid peroxidation is caused by hydroxyl radical (OH·) derived from elevated superoxide anion levels (−Ο2·) (Fig. 3). In turn, hydroxyl radical causes the formation of LOOH. Finally, a variety of reactive lipid aldehydes (RLA) such as malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE) are created, with the ability to modify proteins through protein carbonylation (113,114).
Normally phase I and phase II enzymes would detoxify RLA products, but in individuals exhibiting metabolic syndrome, RLAs accumulate causing damage to cells and their membranes. These alterations have been associated with inflammation and various pathologies including obesity, neurodegenerative disease, asthma, cardiovascular desease (CVD), type II diabetes, and cancer (115–124).
Oxidative stress, as mentioned above, leads to increased free fatty acids concentration in β-type pancreatic cells, enhanced insulin secretion, type II diabetes and cell death, through the exit of cytochrome c from the mitochondria and the activation of caspase 3 (113). One strategy for protection against these detrimental effects has been proposed in a study by Zhu et al (125) in which the effects of perilipin 5 were examined.
Perilipin 5 activates the PI3K/Akt path as well as ERK signaling which activates NRF2β-type pancreatic cells. Subsequently, NRF2 enters the nucleus and as a transcriptional factor activates the antioxidant response element (ARE) that enhances the transcription of down-stream antioxidant enzymes. As a result, β-type pancreatic cells exhibit increased glutathione levels and decreased reactive oxygen species levels. The above signaling pathway thus, enhances β-type pancreatic cell protection, defends them from apoptosis and facilitates the execution of the normal function of these cells.
COVID-19 and obesity
Obesity has been linked to increased susceptibility to infections (126). In addition, a very important field of research suggests that various types of viruses utilize fatty tissue as a reservoir, including adenovirus Ad-36, influenza A virus as well as HIV (127). In this sense, the COVID-19 tissue and cellular localization may be correlated to fatty tissue (128).
The association of obesity with elevated mortality rates compared to non-obese people who have a common virus (H1N1) has been reported (129–133). Another study in 30 people with COVID-19 showed that patients with BMI 27.0±2.5 exhibit the disease with more severe symptoms as compared to patients with BMI 22.0±1.3 (134). Finally, an analysis of BMI correlation in cohort of COVID-19 patients showed that non-survivors who were 15.18% of the total participants, in the respective study had BMI >25 at a rate of 88.2%. On the contrary only 18.9% of survivors, had BMI >25 (135).
Clinical reports of patients infected with SARS-CoV-2 show that several parameters associated with infection as well as the severity of the disease (i.e., older age, hypertension, diabetes, cardiovascular disease) are correlated to viral invasion induced ACE2 down-regulation.
Importantly, angiotensin converting enzyme-2 (ACE2) receptors mediate the entry of SARS-CoV, NL63 and SARS-COV-2 into the cell (136), particularly in type 2 pneumocytes and macrophages, as well as angiotensin II degradation to angiotensin 1–7 via the ACE→Angiotensin II→Angiotensin II receptor type 1 or AT1 receptor axis (137).
Structural, allelic or genetic variations in the SARS-CoV-2 spike protein and genetic or allelic variations of the host receptor ACE2 including rs73635825 (S19P) and rs143936283 (E329G) lead to the cross-species transmission of the virus. The specific modifications have been found to significantly contribute to the susceptibility and/or resistance against the viral infection (138).
Thus, the resulting ACE2 deficiency upon viral invasion may enhance the dys-regulation between the ‘adverse’ ACE→Angiotensin II→AT1 receptor axis and the ‘protective’ ACE2→Angiotensin 1–7→Mas receptor signaling. In the lungs, decreased angiotensin 1–7 and G-protein coupled Mas receptor binding, enhances the severity of vasoconstriction, fibrosis, inflammation, thrombosis and pulmonary damage including edema and permeability triggered by local angiotensin II hyperactivity unopposed by angiotensin 1–7 (139).
Although the association between obesity and heart disease is well-established, underlying pathophysiological processes remain elusive, and it is unclear whether cardiomyopathy in obese patients is due to increased deposition of adipose tissue itself or due to the effects of obesity-associated comorbidities, including hypertension, metabolic syndrome, and diabetes.
In obesity, the heart undergoes structural remodeling and functional alterations leading to obesity-associated cardiomyopathy due to interstitial fibrosis, cardiomyocyte hypertrophy, and cardiac steatosis (140) Oxidative stress, natriuretic peptides, endothelin-1, advanced glycation end products, induction of TGFβ, increased mean arterial pressure in elderly through the activation of the renin-angiotensin-aldosterone system (RAAS) (141), Rho-kinase signaling, leptin-mediated actions, up-regulation of matricellular proteins (such as thrombospondin 1), are molecular mechanisms associated with these processes especially in obese adults (142).
Furthermore, the sleep apnea/obesity hypoventilation syndrome, as well as respective coexisting neurohormonal and metabolic alterations, diabetes (143), insulin resistance and long-term inflammatory adipocyte-derived factors directly influence the pro-inflammatory signaling in the heart (144).
The above data are very important as it seems that lipotoxicity and obesity are directly related to viral infections as well as to the challenges in combating this infection, as shown by the increased need of severely obese patients for ventilator support. The fact that in the western world general population exhibits much higher rates of obesity argues that these countries need to be prepared as regarding intensive care units (ICU) and ventilator devices. Finally, it is important for obese individuals to take all the preventive actions proposed by the WHO to minimize the chances of becoming infected with COVID-19 (145,146).
COVID-19 and the obesity paradox
It is important to note that RAAS and ACE2 are expressed in adipose tissue and that angiotensin II can be released from fat tissue during periods of increased sympathetic nervous system activity with complex interactions linking central RAAS with adipose tissue RAAS (147).
COVID-19 however, seems to challenge the obesity paradox (148) as in various pathologies connected with high levels of inflammation including heart failure, kidney failure and ARDS being obese seems to offer a dose of protection and moderate obese patients tend to present lower mortality.
Indeed, in mechanically ventilated adults with acute lung injury, O’Brien et al (149), in a retrospective study in 1,488 patients, determined that patients with lower body mass index (BMI) were associated with higher mortality as compared to obese patients. In the case of ARDS, it was hypothesized that clinicians tended to admit more readily obese patients to ICU, regarding them as more vulnerable and needing extra care (150). The said obesity paradox was also found to exist for patients with pneumonia according to a meta-analysis of ten cohort studies on mortality (151,152).
Mechanistically, other researchers have expressed the opinion that obesity induces a type of preconditioning to inflammatory cues, constituting obese patients more resistant to the high influx of inflammatory cytokines under ARDS or heart failure conditions.
Indeed, it has been suggested in cardiovascular disease patients that the aforesaid obese may reflect the biological properties of adipose tissue (153). Indeed, not all obese people present inflammation; thus, the terms of metabolically healthy and unhealthy obesity are used with metabolically unhealthy obesity being linked to increased visceral/abdominal fat (76).
Obesity was rarely mentioned in early clinical reports evaluating the clinical risk factors for SARS-CoV-2 infection. Novel data from a single center retrospective study confirm that obesity had a high frequency among patients admitted in intensive care for SARS-CoV-2 requiring invasive mechanical ventilation and that disease severity increased with BMI (154). Indeed, a very recent report on a large sample of patients younger than 60 years tested positive for COVID-19, correlated higher BMIs values with increased probability for admission to critical care (155).
Pregnancy, obesity and COVID-19
Importantly, overweight, pre-pregnancy obese and obese pregnant women are at increased risk for both morbidity and mortality from CMV (156), including all recorded influenza pandemics, 1918 (157), 1957 (158), and 2009 (159), Varicella Zoster (160), Listeria monocytogenes (161), malaria (162), as well as SARS (163). Moreover, the highest mortality risk for these pregnant women was correlated to acute cardiopulmonary conditions presenting in the second and third trimesters (164). Furthermore, the above mentioned pathological conditions were associated with adverse pregnancy outcomes, including preterm birth and fetal death (165).
Maternal burden of coronavirus infection may have significant implications for neonatal immune ontogeny, as high maternal viremia has been associated with significantly lower CD4+ T-cell count in uninfected progeny. Increased levels of pro-inflammatory cytokines produced by placental cells can negatively affect infant innate cytokine responses in early life, pregnancy outcomes and facilitate mother-to-child transmission of coronavirus in the infant. Indeed, increased placenta leptin production affects uterine contractility playing a role in the dysfunctional labor process associated with maternal obesity, and the resultant high cesarean section rates (166).
Pregnancy immune phenotype may be correlated with the SARS-COV-2 prevalence in pregnant women. Both xenobiotics and enveloped viruses such as SARS-COV-2 induce immune-suppression (167) characterized by significant increases in blood phagocytes, placental DCs and immature monocyte-derived DCs, decreases in the number and activity of NK and T cells (168), and inhibition of TH1 responses from maternal-fetal TH2 cytokine cocktail especially IL-1β+IL-6+TNF-α +α-defensins (169) shifting toward Th2 immunity (170), inefficacy of adaptive/inflammatory immunity in the later stages of pregnancy as well as membrane permeabilization to SARS-COV-2 entry (171).
reference link: https://www.spandidos-publications.com/10.3892/mmr.2020.11127
reference link : European Association for the Study of Obesity



{kind=link}