










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Seriously ill COVID-19 patients in African countries are more likely to die than those on other continents, which could be because of a lack of critical care equipment, a study published Friday said.
Africa’s populations have so far been less badly hit by the pandemic than other regions when it comes to total number of cases and deaths—but the authors suggest the mortality rate of those who do get sick could be even higher than their figures suggest because of a lack of data.
“Our study is the first to give a detailed and comprehensive picture of what is happening to people who are severely ill with COVID-19 in Africa,” Bruce Biccard from Groote Schuur Hospital and the University of Cape Town said in a statement.
“Sadly, it indicates that our ability to provide sufficient care is compromised by a shortage of critical care beds and limited resources within intensive care units,” Biccard, who co-led the research, added.
The study followed 3,000 coronavirus patients admitted to intensive care units across 10 African countries between May and December last year.
Almost half of them died within 30 days of admission.
When the researchers compared their findings with corresponding studies from other continents, they found the mortality rate was lower elsewhere.
On average 31.5 percent of critically ill patients died after admission to intensive care in Asia, Europe and the Americas, compared to 48.2 percent in African countries.
Insufficient data
“Poor access to potential life-saving interventions… could be factors in the deaths of these patients, and may also partly explain why one in eight patients had therapy withdrawn or limited,” said Biccard.
The authors estimated that access to treatments such as dialysis and ECMO, a treatment that pumps and oxygenates a patient’s blood outside of the body, was between seven and 14 times lower than what is required to treat severely ill patients.
Unsurprisingly the study also showed that patients with other health issues such as diabetes, AIDS or kidney problems were more at risk of dying than those without.
But noting the limitations of their research, they suggested the situation on the ground could be even worse.
The majority of the 64 hospitals in which the study was conducted were state-funded university hospitals, which are generally better equipped than others.
The study looked at patients in Egypt, Ethiopia, Ghana, Kenya, Libya, Malawi, Mozambique, Niger, Nigeria and South Africa.
Some of these—in particular Egypt and South Africa—are among the better medically resourced countries on the continent.
But the economic cost has been devastating, and the slow vaccine rollout has raised fears that variants could emerge on the continent that would hit Africans and then spread worldwide.
A viable alternative therapy in the management of COVID-19 is phytomedicine. The use of traditional medicine has a long history in nature. Since antiquity, plant resources have contributed immensely to health and medicine. The various secondary metabolites they possess have made them medically useful.
Herbal medicine is predominantly utilized in countries like China, India, Egypt and many others on the African continent for the treatment of several (mild and severe) ailments and infectious diseases, including coronavirus infections (Jin et al. 2020; Yang et al. 2020).
To date, there is yet no effective, approved therapy or vaccine for the treatment of the COVID-19. This, therefore, stresses the need to find an effective and safe approach for the management of infected patients. Most notably, the aurora of natural product-based drug discovery is emerging and boosting body immunity with validated ethnomedicine remains an innovative therapeutic strategy (Tong and Deng 2020).
The emergence of Artemisia annua (A. annua) and its derivatives as effective therapy against malaria pathogen, Plasmodium falciparum, has led to transverse researches exploring newer and diverse pharmaceutical potentials of A. annua extracts and its artemisinin derivatives (Liu et al. 2019; Zyad et al. 2018).
Notably, the outbreak of COVID-19 pandemic, its global human-to-human transmission curve, and the resultant mortality rate have beamed attention on the viability, safety, and efficacy of Artemisia and its derivatives as a potential therapeutic drug for the treatment of SARS-COV-2.
Very recently, some African countries have reportedly claimed that the anecdotal use of an extract of A. annua is efficacious for COVID-19 management, albeit with no scientific evidence demonstrated. In ethnobotanical practice, the whole plant is commonly used for treating malaria, cough, and cold (Nigam et al. 2019). A practice that could likely be based on the recommendation of artemisinin as a component of ACT (artemisinin-combination based therapies) for malaria by the World Health Organization (WHO 2015).
In a recent study, Boukhatem and Setzer (2020) reviewed the antiviral potentials of some aromatic herbs, medicinal plant-derived essential oils, and phytochemicals including Artemisia against various coronaviruses. The isolated pure compounds are known for their immune-modulating and pro-inflammatory host response enhancing properties. It should be noted that Artemisia plants contain several essential oils and bioactive chemical components (Martínez et al. 2012), which broadens their biological activity beyond antimalarial function. While they are widely spread across various continents (particularly in Asia and Africa), they possess an appreciable amount of nutritional values and several health benefits (Brisibe et al. 2009; Nigam et al. 2019).
Remarkably, the broad range of bioactive components in A. annua forms a frontline basis of its adoption as an antiviral drug and therapeutic option against coronavirus infection. Interestingly, it has a high accumulation of minerals (Table 1) as reported by Poisson-Benatouil (2020) including potassium, essential amino acids and low sodium content (Ferreira; IqbalHussain and Khattak 2011).
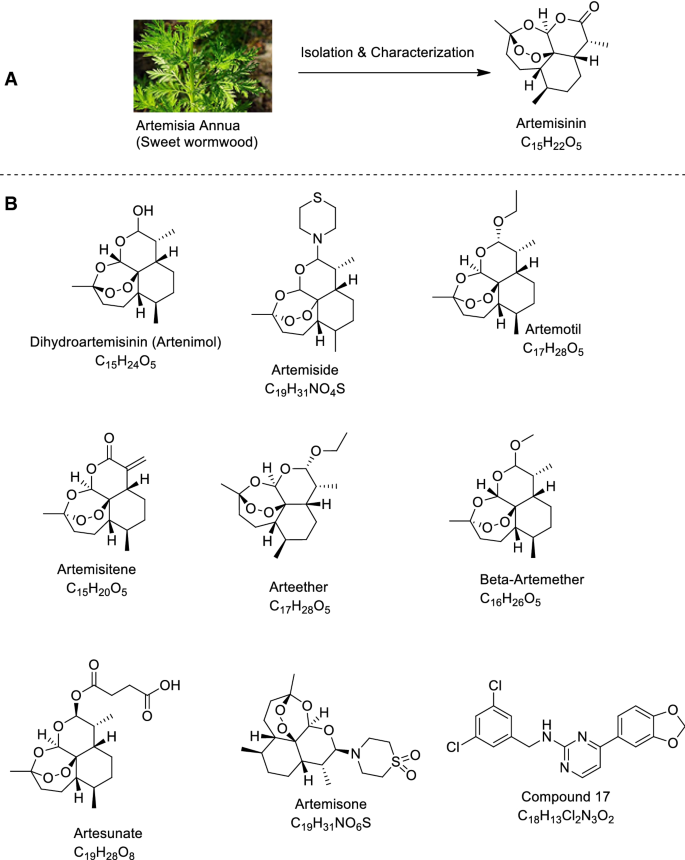
Also, there have been some indications to repurpose Artemisinin, a sesquiterpene lactone derivative of Artemisia (Fig. 1a) as well as other semi-synthetic derivatives (principally Artemether, Arteether and Artesunate) (Fig. 1b) to stem the debilitating effect of COVID-19.
Consequently, a detailed review is significantly needed to give an overview of the anti-coronavirus effect exhibited by Artemisia and Artemisia-based products as well as to motivate further research on the drugs especially as it has been projected that COVID-19 infection may remain for several years. This paper therefore reviews recent literature on the biochemical, pharmacological and safety profiles of Artemisia and Artemisia-based products in the management of COVID-19.
Table 1 High concentration minerals present in Artemisia annua and their functions for human coronavirus disease 2019 management
From: Artemisia and Artemisia-based products for COVID-19 management: current state and future perspective
| Mineral | Functions |
|---|---|
| Zinc | Stimulates and boosts adaptive immune system against coronavirus, increases CD4 level and type 1 T helper cells, inhibits the activity of SARS-CoV-2 enzyme (papain-like protease), improves the production of interferon-α involved in innate immunity, acts as an antioxidant, involves in the metabolism of proline by inhibiting its intracellular transport, inhibits nitric acid production |
| Gallium | Reduces the production of interleukin-6, TNF-α, and other forms of cytokines responsible for inflammatory reactions |
| Selenium | Lowers interleukin-8, regulates the concentration of interleukin-2 and stimulates CD4 lymphocytes |
- Source: Poisson-Benatouil (2020)
Research methodology
This review presents an overview of scientific contributions on Artemisia and Artemisia-based products in the management of COVID-19 including clinical trials and safety information. Scientific articles and reports on Artemisia and Artemisia-based products for the management of SARS-CoV-2 were carefully accessed from online databases such as Google Scholar, PubMed, NCBI, Researchgate COVID-19, ScienceDirect, SciFinder, Web of Science and other scientific databases on COVID-19 such as WHO situation reports on COVID, US National Library of Medicine and Chinese clinical trial registry were also accessed using the keywords; Artemisia, Artemi, SARS-CoV-2, COVID-19. Also, Chem-Draw Ultra 8.0 (Cambridge Soft, 100 Cambridge Park Drive, Cambridge MA 02140) was used for drawing chemical structures.
Origin and bioavailability of Artemisia
The genus Artemisia commonly known as Sagebrush, wormwood, and Sagewort belongs to the largest flowering plants family Asteraceae. This genus is represented by small herbs and shrubs of vascular plants, annual or perennial, with a strong and pleasant aromatic smell, and consists of about 500 species distributed across Africa, Asia, Australia, Europe, Central and South America with 186 species (82 of them endemics) in China.
They can survive in the temperate climates of both hemispheres, usually in dry or semiarid and wetland habitats, while exhibiting various life forms (Martín et al. 2003; Wright 2001; Yu and Zhong 2001). Also, they are largely cosmopolitan, inhabiting from sea level, and often landscape dominating. It is distributed across all continents except in Antarctica (Fig. 2), where no member of the Asteraceae exists (Funk et al. 2005).

Records suggest that the genus Artemisia L. originated from Asia in the temperate, Arid and semi-arid regions during the Cenozoic era (about 66 mya). The centre of diversity was reported to be within the temperate regions of Eurasia and North America by Ling (1982). However, the greatest centre of diversity lies around the temperate areas of Asia with about 38% of the total species population.
In Asia, the centre of origin for Artemisia L. was most probably in the mountain regions of north-western Asia, and diversification and development in the genus were possibly at a peak in the Cenozoic (Wang 2004). Artemisia species have a global widespread within the Asian continent leading in terms of diversity with about 82 of them endemic to China, 50 in Japan, about 35 in Iran (Table 2).
Table 2 The distribution of Artemisia species in Asia and Europe
From: Artemisia and Artemisia-based products for COVID-19 management: current state and future perspective
| S. no | Country | Continent | Number of species | References |
|---|---|---|---|---|
| 1 | China | Asia | 186 | Hu (1965) |
| 2 | Japan | Asia | 50 | Kitamura (1939), Kitamura (1940) |
| 3 | Iran | Asia | 35 | Naghavi et al. (2014) |
| 4 | Pakistan | Asia | 25 | Ghafoor (2002) |
| 5 | Russia | Europe | 174 | Poljakov (1961) |
| 6 | Turkey | Europe | 21 | Kurşat et al. (2015) |
The genus is ecologically and economically significant with an age-long practice for different ethnobotanical usage such as medicinal herbs, source of food in different parts of the world, herbage for feeding livestock, and habitat (in steppe communities).
The plant genus has a well-documented medicinal use with drugs like artemisinin, originally from A. annua, and presently isolated in the aerial part of about 12 species [such as A. bushriences], widely used as drugs and other pharmacological activities (Mannan et al. 2010; Martínez et al. 2012).
They also possess notable economic status as aromatic and medicinal plants with ethnopharmacological properties owing to the different biological activities, including antimalarial, anti-inflammatory, immune-modulating and antioxidant activity (Khlifi et al. 2013; Kim et al. 2015; Woerdenbag et al. 1990).
Essential oils in Artemisia
Essential oils are compounds usually networked or multiplexed with volatile molecules such as terpenes and aromatic components that are phenol derivatives. They have a broad spectrum of bioactivity due to the presence of several active ingredients or secondary metabolites with varying modes of action, which make them play vital roles in nature, ranging from antibacterial, antiviral, antifungal, etc. (Dhifi et al. 2016).
Artemisia species are an excellent source of essential oils such as pinene, thujyl alcohol, cadinene, phellandrene, thujone, etc. and have been reported to achieve remarkable success for several biological activities including, analgesic, anti-coccidial, anti-diabetic, antifungal, antiviral, anti-herpes virus, and lots more (Kumar and Kumari 2018; Martínez et al. 2012).
Anti-viral and immune-stimulatory potentials of Artemisia and Artemisia-based Products against SARS-CoV-2
Artemisia spp. had earlier been reported to consist of essential phytochemicals that contribute to its inhibitory role against viruses (Bora and Sharma 2010). Before the outbreak of COVID-19, some ethnopharmacological studies on Artemisia derivatives revolved around their retroviral properties (Efferth 2018; Jana et al. 2017; Laila et al. 2019; Lubbe et al. 2012), capacity to minimize the replication of herpes viruses (Efferth et al. 2008; Milbradt et al. 2009; Naesens et al. 2006; Nagamune et al. 2007) and inhibition of hepatitis B and C viruses (Dai et al. 2016; Paeshuyse et al. 2006; Qi et al. 2013; Romero et al. 2005), etc. Noteworthily, the bioactive constituents present in A. annua have demonstrated activity against several viruses such as bovine viral diarrhoea (Romero et al. 2006), Epstein-Barr Virus, and Hepatitis B Virus (Haq et al. 2020).
Earlier, some authors reported the use of A. annua against SARS coronavirus which appeared in 2002 Lin et al. (2003). The presence of flavonoids, quercetin, and di-caffeoylquinic acid in the plant inhibits the activity of MERS-CoV-3 CLPro, an enzyme that is similarly produced by SARS-CoV-2 (Jo et al. 2019, 2020).
Interestingly, in a Vero cell-based, 3-(4,5-dimethylthiazol-2-yl-)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium inner salt (MTS) assay for virus-induced cytopathic effect (CPE) screening analysis of medicinal plant extracts with antiviral potentials against SAR-CoV viral strain (α-coronavirus), A. annua alongside three other plants demonstrated a substantial inhibitory effect (Li et al. 2005).
The results showed that A. annua, a highly efficacious species demonstrated a CC50 of 1053.0(± 92.8) µg/ml and EC50 of 34.5 ± 2.6 µg/mL with a selective index > 31 as compared to interferon-α that was > 100,000(± 710.1) and 660.3(± 119.1) respectively, indicating its ability to inhibit SARS-CoV-2 penetration and replication.
Since its discovery as an antiviral agent by a Chinese scientist (Qian et al. 1982), several studies have revealed the promising role of Artemisinin and its derivatives in the inhibition of viruses (Efferth et al. 2008). Artemisinin has been revealed to inhibit replication and penetration of viruses both in vivo and in vitro as well as generating enhanced host type I interferon response (Wang et al. 2020a).
The replication of Hepatitis C replicon, a single-stranded RNAvirus just like SARS-CoV-2 was reported to be inhibited by artemisinin (Obeid et al. 2013). Very recently, a study on molecular dynamic using computer-aided drug discovery (CADD) revealed that artemisinin and its derivatives could be more potent than hydroxychloroquine (HCQ) in silico.
In addition to that, artemisinin and its derived molecules showed an extra mode of interaction by binding to Lys353 and Lys31-binding hotspots of SARS-CoV-2 spike protein and producing a better Vina docking score of − 7.1 kcal/mol for artenilic acid than − 5.5 kcal/mol for hydroxychloroquine (Sehailia and Chemat 2020).
The study further revealed that the formed complexes interfered and remained stable on the SARS-CoV-2 Spike protein receptor site. Besides the antiviral activity, Artemisia contains a high concentration of zinc, which is reported to be effective for the immunomodulation effect of host response and increase in CD4 level (Honscheid et al. 2009). It should be noted that the antioxidant ability of Artemisia enhances immune defense.
Clinical interventional studies of Artemisia and Artemisia–based products as mono- or combined therapy in the face of COVID-19
From a safety point of view, hundreds of phytochemicals present in A. annua have been revealed to be below recommended toxicity limits (Duke 1992; Lutgen 2019; Yang et al. 2010). Some antiviral agents including repurposed off-label drugs such as CQ, HCQ, Redmesivir, etc. have been in the spotlight as frontline therapies for COVID-19 (Bolarin et al. 2020).
However, some of them have demonstrated cardiotoxicity concerns among many other after-administration side-effects (Yang et al. 2010). Notably, Artemisinin has been reported to possess a better and lower toxicity profile compared with CQ and HCQ (Cheong et al. 2020). As such, clinicians can have minimal worries should higher dosage application become necessary. Also, its flexibility as a combination therapy with other drugs suggests its potential usage for the treatment of patients with cases of co-infections.
As of 19th of October 2020, only nine treatment intervention trials on Artemisia spp. and Artemisia products have been registered worldwide for COVID-19 (using Artemisinin, Artesunate, and COVID-19 as search notes) (ClinicalTrials.gov 2020). Six of these were registered in the United States National Library of Medicine while the other three appeared in the Chinese clinical trial registry (ChiCTR 2020), of which one is suspended (ChiCTR2000030082).
Up to date, there exists only a randomized, double-blinded, placebo-controlled, parallel, multi-arm, multi-centre and phase II clinical trial (but not yet recruiting) on Artemisia annua herbal medicine (NCT04530617), which is hypothesized to give improved clinical outcomes in high-risk COVID-19 infected patients when introduced as an early intervention.
The intervention of the study includes; tea 225 mg/1350 mg per day. Oral, one 8 oz brewed tea (two bags) three times a day, Day 1–14. The investigations are focused on evaluating the safety and efficacies on morbidity of COVID-19 patients (adults with mild symptoms) in decreasing the course of the disease and viral load in symptomatic stable positive swab COVID-19 patients (ClinicalTrials.gov 2020).
More clinical interventional studies need to be conducted to further provide therapeutic protocols to substantiate the safety and efficacy of Artemisia and Artemisia products. The potential management of outpatients with COVID-19 and high-risk factors such as cardiovascular diseases needs to be ascertained using Artemisia and its products.
Furthermore, clinical validation of the use of Artemisia either in mono-therapeutic form or as combination therapies with existing drugs, particularly with repurposed drugs of debatable safety profiles is vital. The registered clinical trial interventions using Artemisia annua and Artemisia-based products in mono or combination therapy for COVID-19 treatment are presented in Table 3.
Table 3 Registered clinical trial interventions using Artemisia spp. and Artemisia derivatives in mono- or combination therapy for COVID-19 treatment
From: Artemisia and Artemisia-based products for COVID-19 management: current state and future perspective
| Clinical trials ID | Number of enrolment | Intervention/age | Control | Method/study type | Status (phase) | Study completion date | Location |
|---|---|---|---|---|---|---|---|
| ChiCTR2000033049 | 160 | Artemisinin-pipequine tablets/ 18–65 years old | N/A | Single arm/interventional study | Ongoing (Phase 4) | 19 May–31 December, 2020 | China |
| ChiCTR2000032915 | 240 (120 inintervention and control group each) | Artemisinin-pipequine tablets/2–65 years old | Symptomatic treatment with non-viral drugs | Randomized, parallel/interventional study | Ongoing (Phase 4) | 7 May–31 December, 2020 | China |
| ChiCTR2000030082 | 40 (20 in intervention and control group each) | Dihydroartemisinin piperaquine tablets (each containing 40 mg dihydroartemisinin and 320 mg piperaquine)2 tablets bid for 7 days /18–80 years old | α-Interferon (5 million U bid atomization) + ardibdol (0.2 tid) 7 days | Randomized, parallel/interventional study | Suspended (Phase 4) | 23 February–30 April, 2020 | China |
| NCT04530617 | 360 | tea 225 mg/1350 mg per day. Oral, one 8 oz brewed tea (two bags) three times a day, Day 1–14/18 years and other | placebo | Randomized, parallel, multicentre, multi-arm /interventional study | Ongoing (Phase 2) | September 2020–February 2021 | Mexico |
| NCT04387240 | 22 | Artesunate 100 mg once daily for 5 days/18–60 years old | placebo | Double blinded controlled, randomized, parallel/interventional study | Ongoing (Phase 2) | June–December 2020 | Saudi Arabia |
| NCT04475107 | 76 | Pyronaridine (180 mg)-Artesunate (80 mg)/19 year old and older | placebo | Multi-center, randomized, double-blinded, parallel/interventional study | Ongoing (Phase 2) | July–February, 2021 | Korea, Republic of |
| NCT04532931 | 250 | Arm 1: Standard of care + 2 tablets (200/540 mg artesunate/amodiaquine) daily for 3 days Arm 2: (i) Weight 45 to ≤ 65 kg -Standard of care + 3 tablets (540/180 mg pyronaridine-artesunate) daily for 3 days (ii) Weight ≥ 65 kg–Standard of care + 4 tablets (720/240 mg pyronaridine-artesunate) daily for 3 days/18–65 years old | Standard of care (Paracetamol)–2 tablets (1000 mg)to be taken 6 hourly as needed | Single center, randomized, multi-arm, open-label, parallel/interventional study | Ongoing (Phase 2) | September 3–January 2020 | South Africa |
| NCT04382040 | 50 | ArtemiC (a medical spray comprised of Artemisinin (6 mg/ml), Curcumin (20 mg/ml), Frankincense (= Boswellia) (15 mg/ml) and vitamin C (60 mg/ml) in micellar formulation) sprayed orally twice a day for the first 2 days in the treatment period/ 18 years old and older | placebo | Randomized, parallel/interventional study | Completed (Phase 2) | May 8–July 31 2020 | Israel |
| NCT04502342 | 20 (10 in each group) | i. Cospherunate (50 mg Artesunate/125 mg Amodiaquine) at the rate of 2 tablets orally twice daily for 6 days and Azythromycine 250 mg orally at the rate of 2 tablets the first day, then one tablet for 5 days ii. Cospherunate (50 mg Artesunate/125 mg Amodiaquine) at the rate of 2 tablets orally twice daily for 6 days and Phytomedicine tablet 350 mg at the rate of 2 tablets orally twice daily for 6 days, and Azythromycine 250 mg orally at the rate of 2 tablets the first day, then one tablet for 5 days/18 years and older | N/A | Randomized, open-label | Ongoing (Phase 2) | June 1–September 30, 2020 | Guinea |
- Source: ClinicalTrials.gov (2020)
Mechanistic action of Artemisia and Artemisia-based products on SARS-CoV-2
At present, the use of herbal medicine remains debatable worldwide; it is supposedly believed that they are associated with complications and adverse effects (Wang et al. 2020b). Their acceptability for COVID-19 management is based on the understanding of their mechanism of action (which is derived from experimental and predicted targets of their active chemical ingredients) and clinical profiles.
These two important conditions are largely predicated on the knowledge and clinical profiling of the activities of the chemical ingredients isolated from the plant as described by Jiang et al. (2020). which are, therefore, useful for the following: One, molecular docking and target binding studies in target assessment (Huang et al. 2020).
Two, multi-omics studies for finding clinically-relevant target (Wang et al. 2020b). Three, facilitating molecular and disease network analysis concerning the experimental and predicted targets for understanding the network pharmacology (Yang et al. 2020). Four, facilitating the statistical frequency of appearance analysis of literature-reported chemical ingredients and mechanisms for focusing on the high confidence mechanisms (Huang et al. 2020).
Generally, the mode of action of active ingredients from natural products against coronaviruses is through suppressing virus infection which in turn reduces the viral load (Jassim and Naji 2003). Specifically, the mode of action of A. annua on Spike protein of the SARS-CoV-2 is not clearly understood.
Nevertheless, it has been reported to be by inhibiting the enzymatic activity of chymotrypsin-like protease (3CLpro) (Law et al. 2020). A. annua stimulates adaptive immunity by generating CD8 and CD4 lymphocytes responsible for the production of antibodies targeting SARS-CoV-2 and down-regulating the production of pro-inflammatory cytokines prostaglandin E2 (PGE2), TNF-α, interleukin-6 (IL-6), interleukin-10 (IL-10), thus increasing CD4 count and CD4/CD8 ratio (Poisson-Benatouil 2020). Cytokine storms decrease the number of Treg cell in COVID-19 infected patients, and leads to functionally exhausted CD8 and CD4 lymphocytes which ultimately affects human immune systems and cause severe respiratory failure (De Biasi et al. 2020).
Conclusion and perspective
The antiviral activity of Artemisia and its derivatives against SARS-CoV-2 have been extensively reviewed. Besides its antiviral activity, Artemisia is a super accumulator of zinc and has a well-known toxicological profile (Honscheid et al. 2009). Understanding the safety and efficacy when administered either as a monotherapy or combination therapy, mechanism of action, formulation and active dosage for COVID-19 drug development is required.
We, therefore, recommend sufficient clinical interventional controlled-evidences to elucidate the most effective scheme of administration before integrating both Artemisia herbal medicine and Artemisia products into medicinal practice. Combined administration of Artemisia herbs or other Artemisia products with other antiviral or repurposed drugs should be conducted with stringent adherence to health protocols and clinical guidelines under the supervision of a medical practitioner to understand the drug-drug interaction and assess their effect on pro-inflammatory cytokines and hACE2 receptor.
reference link : https://link.springer.com/article/10.1007/s13596-021-00576-5



{kind=link}