












 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The research team of Gero, a Singapore-based biotech company in collaboration with Roswell Park Comprehensive Cancer Center in Buffalo NY, has presented a study in Nature Communications on associations between aging and the loss of the ability to recover from stresses.
Recently, scientists have reported the first promising examples of biological age reversal by experimental interventions. Indeed, many biological clock types properly predict more years of life for those who choose healthy lifestyles or quit unhealthy ones, such as smoking.
The emergence of big biomedical data involving multiple measurements from the same subjects brings about a whole range of novel opportunities and practical tools to understand and quantify the aging process in humans.
A team of experts in biology and biophysics presented results of a detailed analysis of dynamic properties of the fluctuations of physiological indices along individual aging trajectories.
Healthy human subjects turned out to be very resilient, whereas the loss of resilience turned out to be related to chronic diseases and elevated all-cause mortality risks. The rate of recovery to the equilibrium baseline level after stresses was found to deteriorate with age. Accordingly, the time needed to recover was getting longer and longer.
Being around two weeks for 40-year-old healthy adults, the recovery time stretched to six weeks for 80-year-olds on average in the population. This finding was confirmed in two datasets based on two kinds of biological measurements – blood test parameters and physical activity levels recorded by wearable devices.
“Calculation of resilience based on physical activity data streams has been implemented in the GeroSense iPhone app and made available for the research community via web-based API,” said the first author of the study, Tim Pyrkov, head of the mHealth project at Gero.
If the trend holds at later ages, the extrapolation shows a complete loss of human body resilience, that is the ability to recover, at some age around 120 to 150 years. The reduced resilience was observed even in individuals not suffering from major chronic disease and led to the increase in the range of the fluctuations of physiological indices.
As we age, more time is required to recover after a perturbation, and on average, we spend less and less time close to the optimal physiological state.
The predicted loss of resilience even in the healthiest, most successfully aging individuals, might explain why we do not see an evidential increase of the maximum lifespan, while the average lifespan was steadily growing over recent decades.
The divergent fluctuations of physiological indices may mean that no intervention that does not affect the decline in resilience may effectively increase the maximum lifespan and hence may only lead to an incremental increase in human longevity.
Aging in humans is a complex and multi-stage process. It would, therefore, be difficult to compress the aging process into a single number, such as biological age. Gero’s work shows that longitudinal studies open a whole new window on the aging process and produce independent biomarkers of human aging, suitable for applications in geroscience and future clinical trials of anti-aging interventions.
“Aging in humans exhibits universal features common to complex systems operating on the brink of disintegration. This work is a demonstration of how concepts borrowed from physical sciences can be used in biology to probe different aspects of senescence and frailty to produce strong interventions against aging,” says Peter Fedichev, co-founder and CEO of Gero.
Accordingly, no strong life extension is possible by preventing or curing diseases without interception of the aging process, the root cause of the underlying loss of resilience. We do not foresee any laws of nature prohibiting such an intervention. Therefore, the aging model presented in this work may guide the development of life-extending therapies with the strongest possible effects on healthspan.
“This work by the Gero team shows that longitudinal studies provide novel possibilities for understanding the aging process and systematic identification of biomarkers of human aging in large biomedical data. The research will help to understand the limits of longevity and future anti-aging interventions.
What’s even more important, the study may help to bridge the rising gap between the health- and life-span, which continues to widen in most developing countries,” says Brian Kennedy, distinguished professor of biochemistry and physiology at National University Singapore.
“This work, in my opinion, is a conceptual breakthrough, because it determines and separates the roles of fundamental factors in human longevity—aging, defined as progressive loss of resilience, and age-related diseases, as ‘executors of death’ following the loss of resilience.
It explains why even most effective prevention and treatment of age-related diseases could only improve the average but not the maximal lifespan unless true antiaging therapies have been developed,” says prof. Andrei Gudkov, Ph.D., sr. vice president and chair of the Department of Cell Stress Biology at Roswell Park Comprehensive Cancer Center, a co-author of this work and a co-founder of Genome Protection, Inc., a biotech company that is focused on the development of antiaging therapies.
“The investigation shows that recovery rate is an important signature of aging that can guide the development of drugs to slow the process and extend healthspan,” commented David Sinclair, Harvard Medical School professor of genetics.
“The research from Gero surprisingly comes to a similar quantification of human resilience – a proposed biomarker of aging – based on two very different kinds of data: blood test parameters and physical activity levels recorded by wearable devices. I’m very excited to see how Person-generated Health Data, including data from commercial wearables, can help create individual, longitudinal profiles of health that will be instrumental to shed light on lifetime-scale health phenomena, such as aging,” said Luca Foschini, co-founder and chief data scientist at Evidation Health.
The authors characterized the dynamics of physiological parameters on time scales of human lifespan by a minimum set of two parameters.
The first is an instant value, often referred to as the biological age, and is exemplified in this work by the Dynamic Organism State Index (DOSI). The quantity is associated with stresses, lifestyles and chronic diseases and can be computed from a standard blood test.
The other parameter – the resilience – is new and reflects the dynamic properties of the organism state fluctuations: it informs how quickly the DOSI value gets back to the norm in response to stresses.
When does aging start?
Age-related changes in physiological parameters start from birth. However, various parameters change in different ways at different stages of life, see, e.g., a previous work by the same authors published in Aging US in 2018).
The data from the Nature Communications work shows that there is a good differentiation between the growth phase (mostly complete by the age of 30 and following the universal growth theory by Geoffrey West and aging. At 40+ years, aging manifests itself as a slow (linear, sub-exponential) deviation of physiological indices from their reference values.
How often should one measure biological age?
Physiological parameters are naturally subject to fluctuations around some equilibrium level. Glucose levels rise and drop after having a meal, the number of sleeping hours is slightly different each day. Yet, one can collect a longitudinal dataset, that is a series of such measurements for the same person, and observe that the average levels are different between individuals. Resilience also requires repeated measurements, since one needs to know exactly when recovery was achieved to calculate the resilience.
Importantly, resilience also provides a convenient guide on how often repeated measurements should be taken. As a rule of thumb, the period of observation required for the robust bioage determination should comprise multiple stress and recovery events.
For the most healthy individuals such an observation period would amount to several months and should increase with age. During that time, a robust bioage determination would require several data points per recovery time, that is ideally one measurement in a few days.
Wearable technology comes into play
In 2021, the only practical way to achieve a high (once-per-day or better) sampling rate is to use mobile/wearable sensor data.
In another paper, the authors have focused on wearable/mobile sensor data. They have built a wearable DOSI, which they called GeroSense, and reported its validation tests in Pyrkov et al. Aging (Albany NY) 13.6 (2021): 7900. GeroSense can be used to compute resilience.
Population study shows that the number of individuals showing signs of the loss of resilience increases exponentially with age and doubles every eight years at a rate matching that of the Gompertz mortality law (the observation by B. Gompertz from 1827, who observed for the first time that the all-cause mortality rate doubles every eight years).
Resilience research developments and gaps
The first human explorations of resilience within psychological frameworks studied children, and later incorporated other stages of life (i.e. young adult, midlife, and finally the elderly) [21,22,23]. This trajectory influenced biomedical and pharmaceutical research to include resilience in theories of health trajectories and overall well-being during old age [24,25,26].
Some researchers have posited that “no generally accepted definition of resilience” exists [27]. While consensus over a common definition for resilience may never be reached across all health fields, there is agreement on its importance to health, and more specifically, gerontology [11, 21, 27, 28].
Current health-based literature indicates that resilience is conceptualized as either a mediator or a moderator in exposure-outcome relationships, deviating from the NAS definition [27,28,29,30,31,32]. For example, in physical domain, clinical studies have examined biomarkers such as musculoskeletal changes (adiposity, muscle mass, grip strength, bone mineral density, body weight, gait velocity), stem cell changes (% COP, COP Lamin A), serum markers (hemoglobin, albumin, oxidation products, antioxidants), metabolic markers (HbA1C), hormonal changes (DHEA, testosterone, Vitamin D), and new inflammatory markers (CRP, IL6, TNFa) [33,34,35,36,37,38,39,40,41].
Other studies have attempted to infer individual resilience by examining behaviors and subjective measurements such as emergency department visits, overnight hospital stays, and perceived pain. But these measure general health rather than an ability to absorb and recover from emerging disruptions [29]. Additionally, metrics used by researchers to quantify resilience do not always align with the outcomes that individuals deem important when adapting to a disruption in health (i.e. biomarkers and objective measures versus psychosocial factors and subjective measures) [42,43,44]. Better metrics are needed for new methodological approaches to coherently assess and model complex human systems.
Clinical studies have examined disease-specific resilience (i.e. Alzheimer’s Disease), focusing on neurobiological divergences or disease recovery (i.e. cognitive reserve, brain maintenance, frailty, function post-surgery) [45,46,47,48,49]. Over time, health fields have expanded aging theories, developing the idea of Successful Aging (SA) [10, 11, 50,51,52], But, SA and SA-based theories overlook common aging-related challenges that can disrupt health such as chronic illness.
Additionally, SA-based theories often infer ‘failure’ if an elderly individual is not aging “successfully” according to a socially constructed definition. Resilience models of aging offer improvements over SA models in their ability to incorporate shocks and stressors beyond normal decline and to be tailored to an individual’s unique strengths and circumstances.
The World Health Organization’s (WHO) model of healthy ageing considers an individual as a product of their intrinsic capacity (i.e. personal characteristics, genetic inheritance, and health characteristics), extrinsic environmental characteristics, and functional ability (i.e. intrinsic capacity, extrinsic environmental characteristics and their interactions) [53,54,55]. Aging is positioned on a trajectory that entails three key periods (i.e. high and stable physical capacity, declining physical capacity, significant loss of physical capacity), within which physical capacity slowly declines as one grows older [53]. Here, resilience enables an individual to maintain high and stable functional ability and intrinsic capacity over their life time for as long as possible [51, 56, 57].
Unfortunately, a lack of consensus around operationalizing resilience has led to weak linkages between concepts and methods [15]. Fragmentation across disciplines has produced domain specific divisions of resilience such as physical, psychological, emotional, cognitive, health, motivational, community, cultural, spiritual, and creative resilience [22].
For example, social resilience is defined as “the ability of groups or communities to cope with external stresses and disturbances as a result of social, political and environmental change.” [58] Individual resilience is similar but focuses on the person instead of group. Community resilience differs, as it is framed as emerging from “a set of networked adaptive capacities” with dynamic attributes such as robustness, redundancy, and rapidity [59, 60].
It aligns more closely to public health definitions of community capacity which focus on not only the cultivation and transfer of knowledge but also community characteristics that affect “the ability to identify, mobilize, and address social and public health problems.” [59, 61]
Thus, gerontology has encountered the same two obstacles that have inhibited resilience measurement in other complex systems: (1) resilience is often conflated with risk analysis and quantitative risk assessment, and (2) resilience knowledge is fragmented across disciplines that do not typically communicate with one another.
Polarized perceptions of old age further complicate matters. At one extreme, old age is viewed as an apocalyptic crisis of immense vulnerability, disengagement, and dependency, leading to a “care of the elderly” perspective. At the other extreme, old age is conceived as an important period of social engagement in which elderly contribute to all levels of society (e.g., capital generation, volunteerism, generativity, and intergenerational support), outweighing social costs with the benefits that they contribute. Neither perspective is wrong, but neither is entirely correct. An effective model of resilient aging requires a compromise between the two views.
A life course perspective can address both views and allows for some commonalities in conceptualizations of resilience [31]. The first commonality is that an individual faces some form of adversity over their life course. The second is that the individual has a positive response after facing adversity [62].
The third is that the goal of resilience is adaptation to adversity [10]. This adaptation may refer to establishing a newly optimal critical function operation, or to resisting the same pathway of downward degradation experienced by others in similar positions.
In Fig. 2, we position aging on a trajectory where physical capacity slowly declines as one grows older. System shocks can precipitate regime changes and thresholds determine an individual’s ability to absorb a shock. Resilience supports an individual’s state of high and stable functional ability and intrinsic capacity over their lifetime for as long as possible.
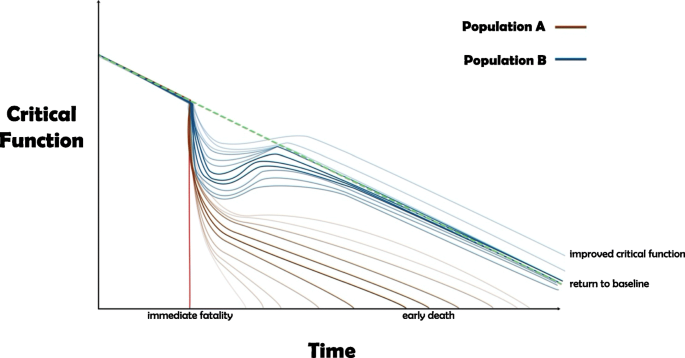
Additionally, in Fig. 2, we show two populations: one comprised of resilient individuals that can recover and the other showing less resilient individuals who demonstrate the tendency of reduced critical functionality and earlier death. Resilience can therefore be understood in relative terms, such that an individual can be deemed more or less resilient than someone else.
Defining threshold values that reflect transitions from one state to another (i.e. robustness, frailty, etc.) can help better inform decision-making about interventions in gerontology and geriatrics and at what point in the trajectory the interventions should be implemented for maximum efficacy and effectiveness. These threshold values can be personalized and retrofitted to an individual’s needs, goals, and outlook on life. Ultimately, degradation to a state of death remains inevitable, so resilience has limitations.
Figure 2 shows two populations of elderly individuals. Population B is comprised of resilient individuals that have the ability to recover, adapt, and return to baseline or close to baseline, with some even improving their critical function. Population A is comprised of less resilient individuals that demonstrate an inability to recover, adapt, and return to baseline, resulting in reduced critical function and earlier death. The blue and brown lines reflect a spectrum of possible trajectories for individuals that are part of Population B and Population A, respectively. The red line signifies a fatality that results in immediate death.
Resilience framing and quantification in gerontology
Quantifying resilience for the elderly using a complex systems perspective can help indicate which sub-populations are better able to recover from disruptions and which populations merit either strengthened protection against disruptions or stronger support should disruptions occur.
Resilience quantifications can also help planners manage disruptions, thereby allowing them to make resilience-informed decisions both during disruptions and in their absence to maximize long-term recovery or investments, respectively. However, there is no gold standard to measure or quantify resilience in aging, and studies are highly variable in definitions, measures and designs [63].
Existing conceptualizations of resilience and healthy aging link to observable and measurable outcomes, albeit inconsistent across studies. Researchers in health fields operationalize aging as a linear process (i.e. latent variable modelling and generalized mixed models), seeking to evaluate the effectiveness of clinical interventions [19, 29, 42, 64, 65].
While linear trends are useful for statistical analyses, aging is a complex, non-linear process that does not necessarily have a clear cause and effect relationship. Moreover, quantitative studies on resilience and aging are conducted using cross-sectional data [62], with few longitudinal studies existing despite their ability to provide greater insights into resilience across the lifespan.
Additionally, benchmarks and thresholds are not consistent across studies. A complex systems perspective is necessary in order to address both upstream and downstream factors that impact life course resilience [13, 66,67,68,69,70].
Complex systems illustrate the interdependent elements within a connected whole, where elements affect one another in subtle ways that can produce cascading effects [71,72,73]. Some studies have begun to examine complex system dynamics in aging by focusing on biological markers and physiological mechanisms of aging or on the general public health system [71, 74,75,76].
However, one model found in the aging and health literature that captures individual and external domains and can help identify inequities between the recovery capabilities of different populations is the socio-ecological model [77, 78] We propose adapting the socio-ecological model (Fig. 3) to a complex systems model for aging resilience, which would allow us to recognize individuals as nested within larger ecosystems and their embedded risks that are beyond their individual control [77, 78].
Furthermore, a complex systems model of resilience can provide quantifiable parameters that account for the different individual and environmental-level spheres of influence observed within existing socio-ecological frameworks. For instance, external factors such as poverty, societal perceptions of race, education, pandemics, and the physical environment can influence the health outcomes of a single individual.
These factors play a larger role as time passes, meaning that they are of critical importance to the elderly [79,80,81,82]. Learning from social scientists, we can begin to incorporate these social determinants of health in quantitative models by using socio-economic, geographic information systems, social support, political, and demographic data [83,84,85,86,87].
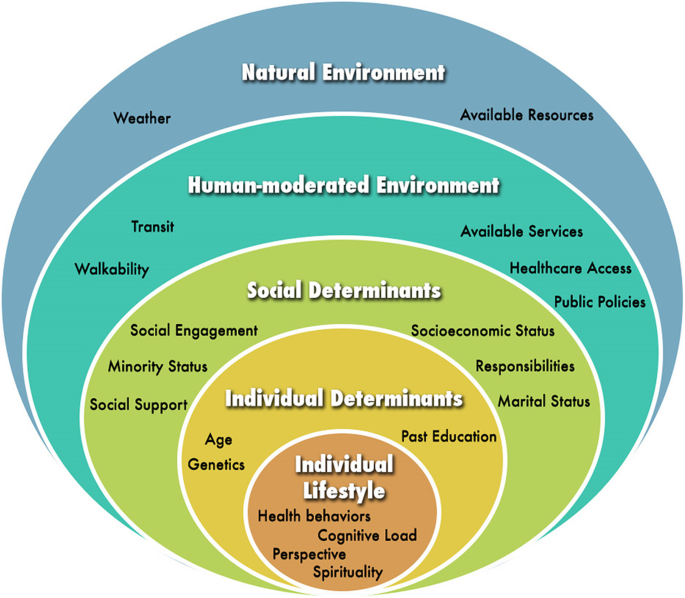
Figure 3 visualizes the socio-ecological model and the five spheres (or levels) of influence (i.e., individual lifestyle, individual determinants, social determinants, human-moderated environment, and natural environment) on health behaviors and outcomes. Individuals are nested within a larger ecosystem and their embedded risks are influenced by factors within and outside of their control at each sphere of influence. This figure was adapted from McLeroy, Steckler, and Bibeau (1988).
Within the socio-ecological framework, five spheres influence an individual’s wellbeing, starting with characteristics of an individual, then expanding outwards to the larger environment. Applied to resilience in older adults, the first sphere embodies individual healthy behaviors such as social engagement and cognitive load. Next, the second sphere includes individual determinants that are outside the individual’s direct control, such as genetics, past education, and socio-economic status that affect how people may experience stressful events [88].
Third, we include the social realm, quantifying elements such as social cohesion and belonging [89,90,91,92,93]. Fourth is the built environment within which aging adults live, including aspects that support the nested systems, such as electricity, access to air conditioning during heat waves, greenspaces for physical activity, and walkability to cafes or grocery stores with fresh produce for healthy meals. Finally, there are changes in circumstances or resources of the natural world, such as pandemics, natural, meteorological, or human disasters [94,95,96,97,98].
These spheres directly impact numerous factors that determine health behaviors and outcomes, such as institutional factors, community factors, public policy (i.e. governance and law-making), intrapersonal factors, and interpersonal processes, and can be used to frame quantifications of individual resilience [99].
For example, recent public health “aging-in-place” [100,101,102,103,104,105,106] (supporting remaining in familiar environments as one ages) and age-friendly community [107,108,109,110,111,112,113,114,115] (environmental policies and practices to reduce barriers to active aging) efforts have attempted to use a broader systems perspective to support the long term resilience of aging adults by using a socio-ecological perspective [102].
The resilience matrix
The components of a resilience approach (preparing, absorbing, recovering, and adapting) encompass the different stages that medical and public health professionals employ for aging individuals and geriatric populations. The different spheres of the socio-ecological model can frame the scale of the resilience analysis.
The resilience matrix (Fig. 4)—first developed by Linkov et al. (2013) and applied in different fields [68, 69, 96, 116]—combines the National Academies of Sciences system functions (plan/prepare, absorb, recover, adapt) with system domains (physical, information, cognitive, social), aligning with the socio-ecological model.
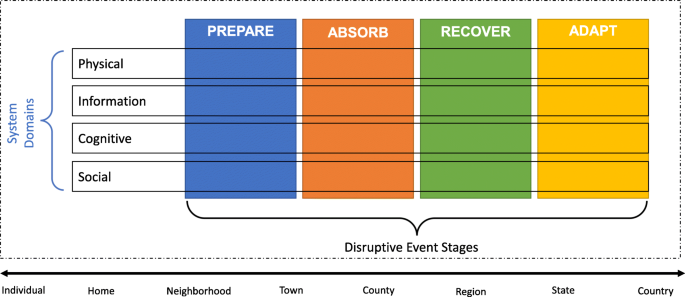
The matrix collects data in the physical realm, and translates it to information to be used for cognitive decision making [117]. These three systems domains encompass the first two spheres of the socio-ecological framework. A fourth systems domain (i.e. social) is overlaid on the socio-ecological social sphere comprising circumstances like reciprocity in social relationships, or social isolation. Thus, the resilience matrix examines resilience as instigated by the individual’s agency on an individual scale, while omitting the larger contextual factors.
The matrix can be used for individuals evaluating their own resilience, while public health officials must navigate the implications of changes in the outermost spheres. For example, individuals and their doctors can target the component of the resilience matrix that emphasizes individual agency over various deterministic features of resilience and health systems. They may also recover from a disruption more effectively through improved formal-care and self-care processes according to the resilience matrix.
The Resilience Matrix shown in Fig. 4 combines the National Academies of Sciences (NAS) system functions and the Network-Centric Warfare domains. The rows of the matrix represent four systems domains that were adapted from the Network-Centric Operations doctrine in Alberts (2001). The columns represent the four stages of resilient systems from the NAS Disaster Resilience Model. The matrix can be applied to different scales, from micro (i.e. individual- or home-level) to macro (i.e. global- or country-level). This figure was adapted from Linkov et al. (2013).
The resilience matrix is constructed using existing research in health fields and by assessing their implications throughout the different stages and domains applied to a geriatric population. Each cell in the matrix include metrics that address the question: “How is the system’s ability to [plan/prepare for, absorb, recover from, adapt to] a health disruption among older individuals implemented in the [physical, information, cognitive, social] domain?” Since most aging metrics are difficult to measure through direct means, they must be estimated using a system-by-system basis that incorporates both quantitative and qualitative measures.
The relevant quantifications are dependent on the scale of the analysis and the scope of the objectives. Physical responses characterize the circumstances of an individual’s body. Informational responses encompass the information and resources available to individuals to help them cope during disruptions. Cognitive responses reflect the individual’s engagement with the changes needed during disruptions.
Social responses encompass the existing structure of the individual’s social network and specifically its ability or willingness to support an individual, including circumstances in which the individual might not be actively engaged in seeking support [118]. Table 1 provides examples of these indicators within the Resilience Matrix. Each cell provides specific examples of indicators and metrics for each domain and stage of resilience that can be used to characterize and quantify resilience among older adults.
Table 1 Resilience metrics for older adults
| Prepare | Absorb | Recover | Adapt | |
|---|---|---|---|---|
| Physical | Good state of health | Functioning systems available to respond | System works to restore lost function | Optimal value of lost function attained or improved upon |
| Metric | Blood pressure, mobility, grip strength etc. | Immune system, other body attributes | Is recovery occurring, are system attributes improving? | Blood pressure, mobility, grip strength etc. |
| Informational | Registered for relevant services and alerts | Identify problems, engage with appropriate agencies to resolve | Use the resources for needed support | Resource management |
| Metric | Number and relevance of services signed up for | Does individual confront and address problems? | Output of resources according to disruption (money, assistance) | Do the resources meet the need over time? |
| Cognitive | Awareness of baseline health and needs | Recognize new challenges and seek information and recommendations | Decision making and behavioral change to respond to new circumstances | Sustained behavioral changes |
| Metric | Is individual aware of events? Does individual know baseline expectations for health? | Does individual recognize and act on emerging problems? | What behavior changes are committed to adjust to new circumstances? | Are the adaptive changes maintained over time? |
| Social | Groups of friends and acquaintances | Social ties engage to ensure individual is reacting to disruption | Social ties provide resources and support | Social ties are retained despite new circumstances |
| Metric | How many people does individual speak to in a week? | How many people contact individual in a week? | How many social ties able to provide support? | Percentage of ties independent of a specific context |
The resilience matrix in Table 1 can characterize resilience within individual control, although the socio-ecological model stresses that many factors influencing well-being are beyond individual control [119]. The stability and benefits of the outmost spheres of the socio-economic framework can reduce the burden of individual-level resilience.
For example, a neighborhood with walkable streets and/or safe green spaces is more conducive to socializing among older people, which can foster social support and combat loneliness. Although resilience may be measured using an individual scale, the externalities of the socio-ecological model reveal opportunities to further enhance and anchor individual resilience within a broader coherent system. Ultimately, all individuals live within a community and are impacted by it, regardless of their level of engagement with it.
reference link: https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-020-01965-2
More information: Longitudinal analysis of blood markers reveals progressive loss of resilience and predicts human lifespan limit, Nature Communications (2021). DOI: 10.1038/s41467-021-23014-1 , www.nature.com/articles/s41467-021-23014-1







{kind=link}