










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



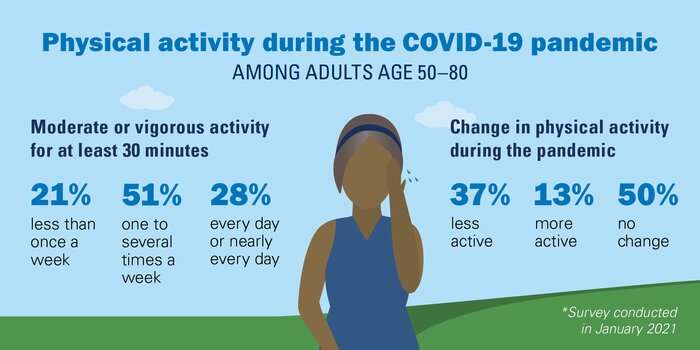
More than a third of people between the ages of 50 and 80 report their physical activity declined in the pandemic’s first 10 months, and more than a quarter say they’re in worse physical condition now than before the pandemic, according to the new findings from the National Poll on Healthy Aging. Many of these adults also reported an increased fear of falling.
Fall research suggests that both reduced physical conditioning and fear of falling can increase future fall risk and reduce independence. As the pandemic eases in the United States, the poll leaders note that better awareness of this connection could help motivate adults of any age to safely increase or maintain their physical activity – especially if they have been less active or mobile due to the pandemic.
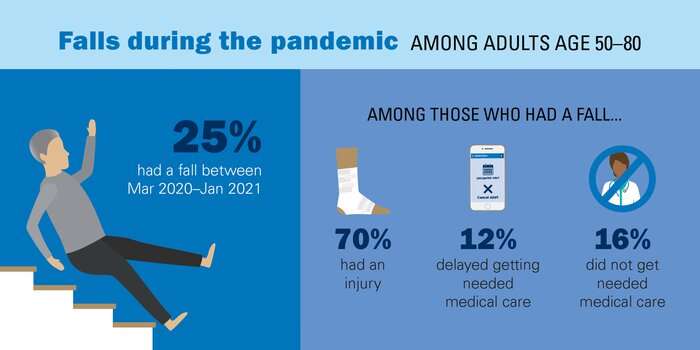
The poll finds 25% of older adults experienced a fall between the start of the pandemic in March 2020 and January 2021, when the poll was conducted. Forty percent of those who experienced a fall had more than one fall during this period.
The poll also points to specific groups of older adults – women, Blacks, older adults experiencing loneliness and adults over age 65 – who may need additional help to improve physical conditioning and reduce fall risk. That help could come from health and fitness providers, and family and friends.
The poll is based at the University of Michigan’s Institute for Healthcare Policy and Innovation and receives support from AARP and Michigan Medicine, U-M’s academic medical center. The new report is based on answers from a national sample of more than 2,000 adults aged 50 to 80 to a poll taken in January 2021.
“Many older adults fall each year, and the pandemic was no exception. Many falls result in at least a minor injury in this age group, and a third require medical attention,” said Geoffrey Hoffman, Ph.D., an assistant professor in the U-M School of Nursing and falls researcher who worked with the poll team.
“Physical conditioning can make a major difference for maintaining independence, including avoiding a fall, but also how well someone reacts to and recovers from one. Focusing on prevention now, including physical health and activity but also home safety and social factors that can increase risk, is crucial.”
Less activity, more fear
More than a third of older adults (37%) reported being less physically active since the pandemic began. Nearly the same percentage said they spent less time on their feet, walking or standing, after March 2020.
This reduced activity translated into 27% saying their physical conditioning – flexibility, muscle strength and endurance – had worsened. Mobility – the ability to move around including with a cane, walker or vehicle – declined in 25%, according to poll responses.
The poll also asked about fear of falling, which was experienced by 36% of respondents overall, and by nearly half of all poll respondents over age 65 (46%) and of women age 50 to 80 (44%).
Among all older adults who said they fear falling, 23% said that fear had increased during the pandemic. But the percentage that reported increased fear of falling was much higher among those who reported less physical activity (32%), worsened physical conditioning (42%) or worsened mobility (45%).
Falls lead to the deaths of more than 32,000 older adults each year, and the number has risen steadily in recent years and is expected to continue to increase with the aging of the US population, according to the Centers for Disease Control and Prevention.
Links with loneliness and delayed care
The poll also reveals clues about how the loneliness and lack of companionship that increased among older adults during the pandemic might play into changes in activity levels, mobility and fall risk, says poll director Preeti Malani, M.D., a Michigan Medicine infectious disease physician also trained in geriatrics.
The percentage of older adults reporting falls was higher – 32% – among those who said they lack companionship. This group was also more likely than others to report less physical activity and worsened mobility and physical conditioning. The NPHA has issued two previous reports on the health aspects of loneliness in older adults, both before and during the pandemic.
“As life gets closer to normal, especially for the large percentage of older adults who are fully vaccinated against COVID-19, health care providers and loved ones should encourage more interactions that involve safe physical activity,” she said.
“We need to make up for lost time and get older adults on track, or back on track, with the kinds of movement and strengthening that can safeguard their independence by reducing their risk of falls or of major fall-related injuries. Even better if this happens in conjunction with social interaction.”
Hoffman and Malani also note another of the poll’s findings: During the pandemic, 28% of the older adults injured by a fall either delayed or did not receive medical care they felt they needed. Forty percent of this group said the pandemic was directly related to this lack of care.
People who have lingering effects from a fall experienced during the height of the pandemic – joint pain or reduced mobility and strength, for instance – should seek rehabilitation and other care to avoid or reduce the risk of any further issues, they add.
“Falls are a significant health and safety concern for older adults,” said Alison Bryant, Ph.D., senior vice president of research for AARP. “Thankfully, there are many ways you can reduce your risk of falling, including simple home modifications like using brighter lightbulbs, removing throw rugs and making sure electrical cords are tucked out of the way.”
AARP offers a free checklist for things older adults and their caregivers can do to prevent falls at home.
The CDC offers a toolkit for older adults and their caregivers, and for health providers, to assist with fall prevention.
The National Poll on Healthy Aging results are based on responses from a nationally representative sample of 2,074 adults aged 50 to 80 who answered a wide range of questions online in January 2021. Questions were written, and data interpreted and compiled, by the IHPI team.
Laptops and Internet access were provided to poll respondents who did not already have them. A full report of the findings and methodology is available at www.healthyagingpoll.org, along with past National Poll on Healthy Aging reports.
This review of the global burden of trauma during the COVID-19 pandemic has shown an overall reduction in the footfall of trauma, with an increase in incidents occurring at home. Whilst COVID-19 negated systemic changes in the delivery of elective surgery68 and cancer care, this study has shown that the care of patients sustaining trauma was largely unchanged during the pandemic.
This may be due to reductions in the absolute numbers of trauma being compensated for by concomitant increases in paediatric trauma, interpersonal violence, DSH, and high energy trauma such as falls from height. Whilst COVID-19 has persisted at the forefront of global healthcare over recent months, the burden of trauma to the health system remains. Multiple studies have been published on how trauma has impacted different regions and healthcare systems around the world, however, the worldwide burden of trauma during this pandemic has yet to be fully determined.
As illustrated in the included studies which compared trauma patients during the COVID-19 pandemic to a matched historical cohort, there has been reported reductions in the absolute numbers of trauma patients by an average of 52.68%. Considering the trauma aetiologies during the pandemic, there has been an increase in the proportion of trauma due to assaults and high-energy falls, as well as a general increase in the proportion of trauma that occurred indoors.
This is coupled with a decrease in other aetiologies including road traffic accidents and sports injuries. This change reflects the lockdown measures put in place. The rise in assaults, domestic violence and non-accidental injury is likely a result of the well documented increase in domestic abuse and alcohol consumption.41,69,70
Falls from less than 2 m continue to be the most common mechanism of injury in trauma, which generally occur in the elderly.71 These injuries tend to occur indoors and therefore the stimulus for such injuries remains unchanged. Furthermore, an increase in falls from height in the paediatric population has been demonstrated, which in part has been attributed to trampoline injuries, and reflects the closure of schools across countries.11
The decrease in road traffic accidents reflects the fall in travel secondary to lockdown measures, and similarly the reduction in sports injuries can be attributed to the cessation of group sports activities as well as closure of gyms, sports clubs and leisure centres. Paradoxically, some studies reported an increase in the proportion of injuries occurring in the street, which may be due to more children and young people spending free time in the street in the absence of scheduled school or work.
Whilst a reduction of trauma patients is a welcome finding to healthcare systems struggling to manage a viral pandemic; it is clear that national lockdown measures can dictate the number and type of trauma seen. Government public health advice and messaging can significantly alter the burden of trauma to health systems across the globe.
It is crucial for government offices to appreciate the impact of their decisions on the distribution of burden to healthcare systems. Equally, public health measures should be considered to minimise the significant increase in trauma due to domestic abuse and alcohol consumption.
Regarding the management of trauma during the COVID-19 pandemic, in general a trend towards a higher proportion of trauma patients undergoing operative management was identified. This may reflect a higher threshold for trauma patients with more ‘minor’ trauma that would have previously been admitted to hospital being managed in primary care or the emergency department, as well as a reluctance for patients to present to hospital in fear of the virus.
Considering management of orthopaedic limb injuries, a slight decrease in the proportion of patients undergoing fracture fixation was identified, however more research is required to ascertain the effects of the pandemic on decision for operative intervention, and comparison between countries. In such cases where surgery is not life or limb saving, there are instances where the risk of surgery in the context of COVID-19 may outweigh the benefits of ‘optimal’ fracture fixation.
This is consistent with guidelines released on fracture fixation in the context of the COVID-19 pandemic, including the British Orthopaedic Associated Standards for Trauma guidelines.8 Indeed, the detrimental outcomes from emergency surgery in patients with COVID-19 has been documented.7
Data from the UK from Park et al. shows a preference towards local or regional anaesthesia prior to surgery.10 Furthermore, the benefits from Wide Awake Local Anaesthesia no Tourniquet (WALANT) surgery in hand trauma are increasingly apparent in the context of the COVID-19 pandemic.19 Increased study in this field from multiple hand trauma centres will give further insight into the effectiveness of this method when used during the pandemic.
National guidelines for the management of fractures during COVID-19 tended towards non-operative management options.8 This is clearly a deviation from current well-established gold standard treatment of fractures in the light of resource re-allocation to treat patients with COVID-19. Many theatre suites were converted to intensive care facilitates to cope with the burden of COVID-19 patients requiring invasive ventilation.
Anaesthetists and other personnel were re-deployed from theatre duties which resulted in a reduced capacity for surgical fixation of fractures. Whilst it is entirely understandable that these changes were made to support the pandemic; it is important for health systems now to utilise data and learnings from the last few months to ensure they are fully prepared for a second wave.
Prioritising the treatment of COVID-19 whilst at the same time striving to provide gold standard treatment for trauma. It is important that the attention and volume of resources directed to dealing with COVID-19 does not indirectly harm other patients, for example patients with active malignancy who face rationing of services and delays to treatment during the pandemic.72, 73, 74
This study is not without limitations. The study is prone to selection bias; however, this was minimised by carrying out a search on multiple databases (Medline, Embase and Cochrane). This was then followed by a backward citation search to review papers sites by each article and a forward citation search to identify any papers not picked up from the initial search.
Furthermore, eligibility assessment of the article was carried out by two independent reviewers and any disagreements were resolved by discussion with the senior author. In addition, due to heterogeneity in outcome measures there was a risk of interpretation bias, but this was minimised by using a standardised proforma for data extraction.
Whilst the number of patients that contracted COVID-19 following admission for trauma appears low from the included studies, these figures may not reflect the true numbers and large variation exists between the number of patients being tested with either antigen or antibody testing.
Furthermore, to date, morbidity and mortality outcomes from trauma in the context of COVID-19 are relatively under-reported. At the present time, whilst lockdown measures are slowly being eased across countries, the threat of the COVID-19 pandemic continues and long-term outcomes remain to be determined.
This scoping review has provided a snapshot of how the presentation and management of trauma has changed during the COVID-19 pandemic. However, its limitations must be acknowledged. Notably, to date there is a lack of evidence in the literature, with the majority of studies looking at small numbers and being retrospective in nature.
Papers investigating solely fragility neck of femur fractures were excluded from this study as this was considered a separate cohort in itself, and therefore the authors would recommend a standalone review for this area.
Conclusions
The COVID-19 pandemic has resulted in a reduction in footfall of patients presenting with trauma. The change in the incidence of trauma aetiologies reflects lockdown measures put in place. However, constraints secondary to the pandemic have not significantly altered the management of these patients. Our data has given preliminary evidence of a shift in the presentation and management of trauma as a result of the COVID-19 pandemic.
This study has given an indication of an imminent increase in trauma caused by assault during the lockdown period, accompanied by a rise in incidents occurring at home. Lastly, our data has shown that the provision of trauma care was not largely altered by the pandemic, in contrast with the changes in the delivery of elective and cancer surgery.
Government and health systems should utilise available data and learnings from this period to establish strategies that optimise trauma care in preparedness for the second wave. Further research is required in order to assess long-term outcomes in these patients.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7666557/
More information: The poll is available at www.healthyagingpoll.org/repor … ng-COVID-19-pandemic



{kind=link}
[…] The rise in seniors falling and injuring themselves increased during the… […]