










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Although there have been many studies into COVID-19, and even studies into the effect of SARS-CoV-2 infection on pregnant mothers, relatively few studies have looked at what impact maternal COVID-19 infection may have on the developing fetus.
They found that, perhaps unsurprisingly, babies born to mothers with recent or ongoing infection had enhanced levels of circulating mediators as well as increased percentages of cells known to be involved in rapid response to infection.
Notably, the ability of immune cells to make mediators was enhanced even in babies born to mothers who had COVID-19 earlier in pregnancy. This suggests that infection in the mother has altered the immune system of the baby.
Commenting on the importance of their findings, Dr. Deena Gibbons said that “this data highlights that the neonatal immune system can be affected by maternal state even in the absence of direct infection of the baby. This opens up many avenues of research and suggest that other maternal factors may be capable of changing fetal immune system development”.
Sarah Gee, first author of the paper and a Ph.D. student in the Peter Gorer Department of Immunobiology, added that “it will be interesting to know whether these immune changes allow the neonate to make better responses to subsequent infections after birth.”
They are also now looking at how maternal infection may be changing the immune system of the infant and how long these changes might remain.
Why are pregnant women susceptible to COVID-19?
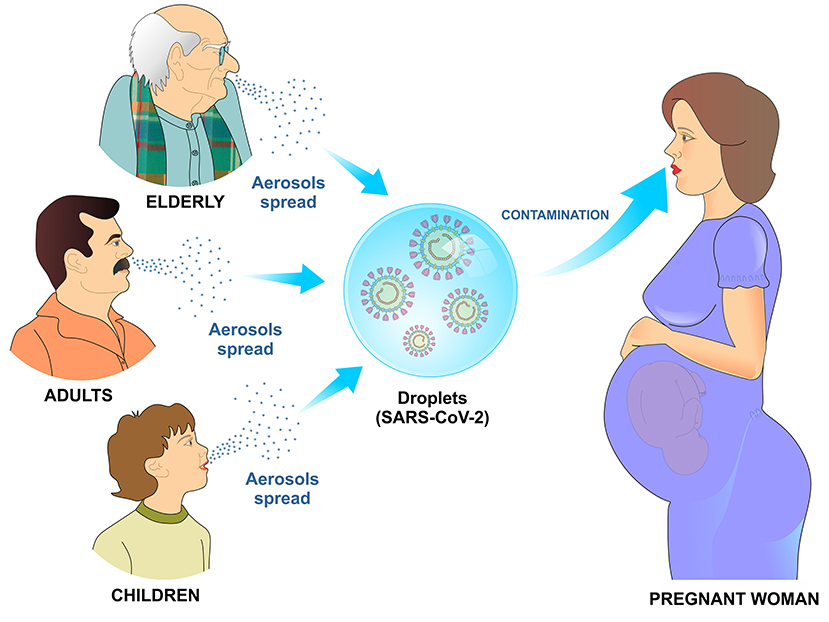
ARS-Cov-2 can infect newborns, children, young adults, pregnant women and elderly (3). This virus is more contagious than the coronavirus that causes severe respiratory distress syndrome (SARS), which had infected ~8,000 people and caused 800 deaths so far. The combination of inadequate immune response and high infectivity can contribute to the SARS-CoV-2 widespread. Contagion occurs mainly through droplets and aerosols spread in the environment by the infected people (1) (Figure 1).
Once in contact with the body, SARS-CoV-2 binds to a cell surface receptor, invades the endosome and eventually fuses viral and lysosomal membranes. In mature viruses, the spike protein is present as a trimer, with three S1 receptor-binding heads, sitting on top of an S2 membrane fusion rod. Like SARS-CoV, SARS-CoV-2 recognizes the angiotensin-converting enzyme 2 (ACE2) as its receptor (4).
During pregnancy, the maternal immune system faces some challenges which includes establishing and maintaining tolerance to the fetus, as well as preserving the ability to fight against viruses and bacteria, therefore, a healthy pregnancy depends on immune adaptations. In fact, the maternal immunological system adapts and changes with the growth and development of the fetus at the different stages of pregnancy, which goes from a pro-inflammatory state (beneficial for embryo implantation and placentation) in the first trimester to an anti-inflammatory state (useful for fetal growth) in the second trimester. In the third trimester, it reaches a second pro-inflammatory state (in preparation for the start of childbirth) (3, 5).
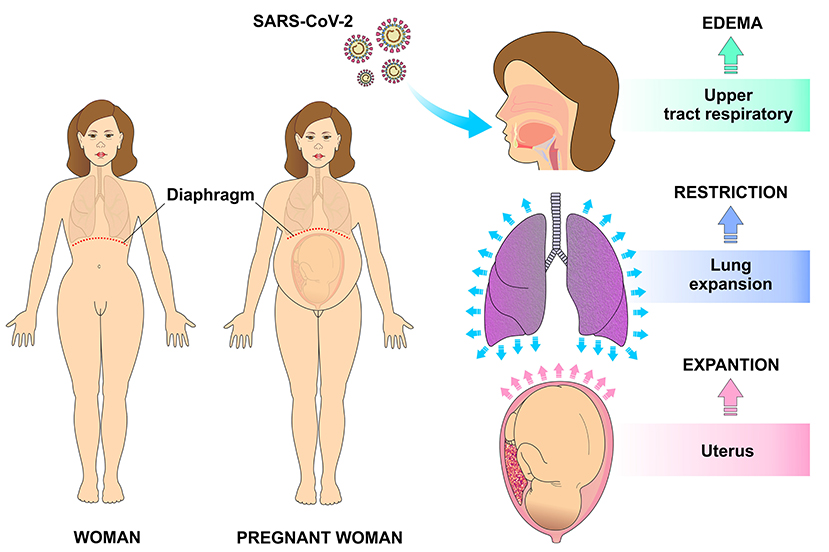
The immune system of a pregnant woman is well-prepared to defend against the invasion of pathogens in such a way that innate immune cells like NK cells and monocytes respond more strongly to viral challenges. On the other hand, some adaptive immune responses are negatively regulated during pregnancy. In addition, the high levels of estrogen and progesterone induce the upper part of the respiratory tract to swell which, in addition to the restricted lung expansion on the last gestational trimester, make the pregnant woman more susceptible to respiratory pathogens such as SARS-CoV-2 (3, 5) (Figure 2).
Previous reports have shown that SARS infection during pregnancy can lead to premature birth, intrauterine growth restriction and spontaneous abortion. However, there is still no strong evidence of vertical transmission of SARS-Cov-2. Therefore, it seems that these complications are caused by the direct effect of this virus on mothers. Although current evidence is limited regarding the transmission of the new coronavirus during pregnancy and lactation, the potential risk of vertical transmission must not be rule out (3, 6, 7).
In this review, the main changes in the immune system that occur during pregnancy, which may increase susceptibility to SARS-Cov-2 infection, are discussed as well as the possible mechanisms involved in the transmission of the virus to the fetus by vertical transmission and during breastfeeding.
Pregnancy, Immunology, and Susceptibility to SARS-COV-2
Human decidua during pregnancy involves a high number of immune cells, predominantly macrophages, natural killer (NK) cells, and regulatory T cells (Treg). During the first trimester of pregnancy, macrophages and natural killer (NK) cells accumulate around the trophoblastic cells, which results in a protective effect, preventing abortion of the allogeneic fetus (33, 34).
The maternal immune system protects the mother from aggressors coming from the environment and prevents damage to the fetus. On the other hand, the fetus activates the immune response that changes the way the pregnant woman responds to the environment, which makes the immune response very unique during pregnancy.
Therefore, this particular immune system must be characterized by a modulated immune condition, rather than a suppressed one (33).
In pregnancy, progesterone has immunomodulatory properties that in addition to preventing the mother from recognizing the fetus as an antigen, it can influence the evolution of autoimmune diseases with improvement in conditions such as rheumatoid arthritis. During pregnancy, there is an increase in anti-inflammatory molecules such as interleukin-1 receptor antagonist (IL-RA) and tumor necrosis factor-α receptor (TNF-R), whereas a decrease in IL-1b and tumor necrosis factor-α (TNF-α) are observed (35).
In the human placenta, the trophoblast expresses pattern recognition receptors (PRRs) that act as sensors to detect external aggressors. Through them, the trophoblast is able to recognize bacteria and viruses, and then secrete cytokines and interferons.
Interferons are potent antiviral proteins that also have important immunomodulatory functions (34, 36). In addition, active transport of antibodies of the IgG class produced by maternal humoral immunity occurs through the placenta after 16 weeks of pregnancy, resulting in increased fetal immunity against microorganisms (34).
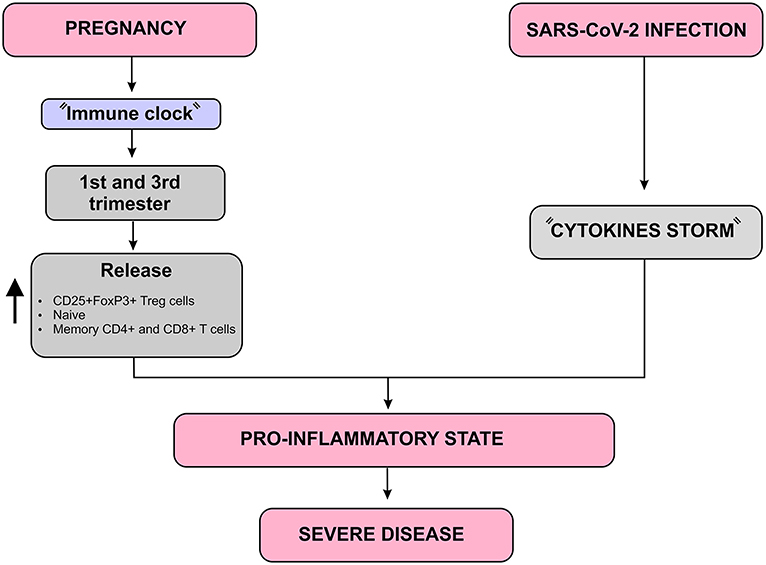
Immunity undergoes some changes during pregnancy that avoids an exacerbated immunological response against the allogeneic fetus, but maintains an adequate immune response against invading microorganisms (3). Aghaeepour et al. described how a “immune clock” occurs during pregnancy through a progressive increase in the release of CD25+FoxP3+ Treg cells, naive and memory CD4+ and CD8+ T cells as well as γδ T cells (37).
Considering that pregnant women are in a pro-inflammatory state in the first and third trimester, the SARS-CoV-2-induced cytokine storm may result in a more severe inflammatory state in these women. In addition, the occurrence of maternal inflammation as a result of viral infections during pregnancy can affect various aspects of the fetal brain and can lead to a wide range of neuronal dysfunctions and behavioral phenotypes (7) (Figure 6).
However, changes in the levels of estrogen and progesterone from the first gestational trimester cause respiratory, cardiovascular and immune changes that make pregnant women more susceptible to SARS-Cov-2 infection, in addition to an increased risk of developing severe acute respiratory syndrome (SARS).
The effect of progesterone on the nasal mucosa facilitates the adhesion of the virus and hinders its elimination. Moreover, the increase in oxygen consumption due to vascular congestion and the decrease in the functional residual capacity of the lung contribute to an increased risk for severe respiratory symptoms in infected pregnant women (38).
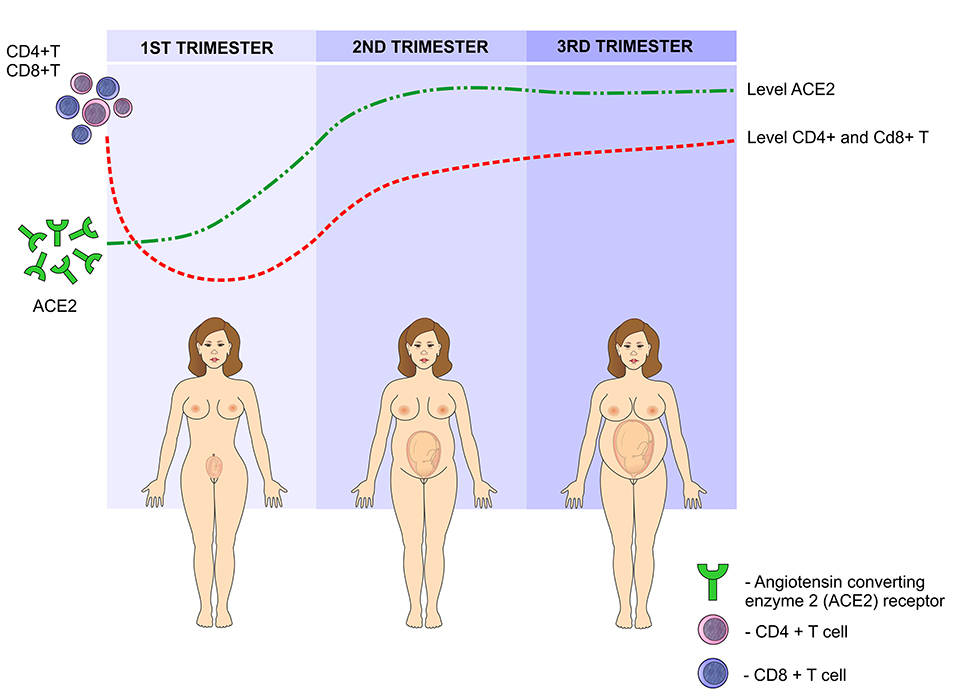
Such changes in the levels of estrogen and progesterone in the first trimester cause a reversible degeneration in the thymus, with a decrease in CD4 + and CD8 + T cells. In addition, the activity of these cells significantly reduces, contributing to a greater susceptibility to infections during pregnancy (38).
Another risk factor involves the angiotensin converting enzyme 2 (ACE2) receptor, to which the virus binds before infecting the cell and it is upregulated during pregnancy. As a result of higher ACE2 expression, pregnant women may be at an elevated risk of complications from SARS-CoV-2 infection (39).
Previous studies have reported an increase in these receptors in the kidneys of pregnant women, which may contribute to the efficient regulation of blood pressure during pregnancy. However, it can favor the binding of the virus and therefore, facilitating its entry into the host’s cells (38) (Figure 7).
SARS-COV-2 in the Postpartum
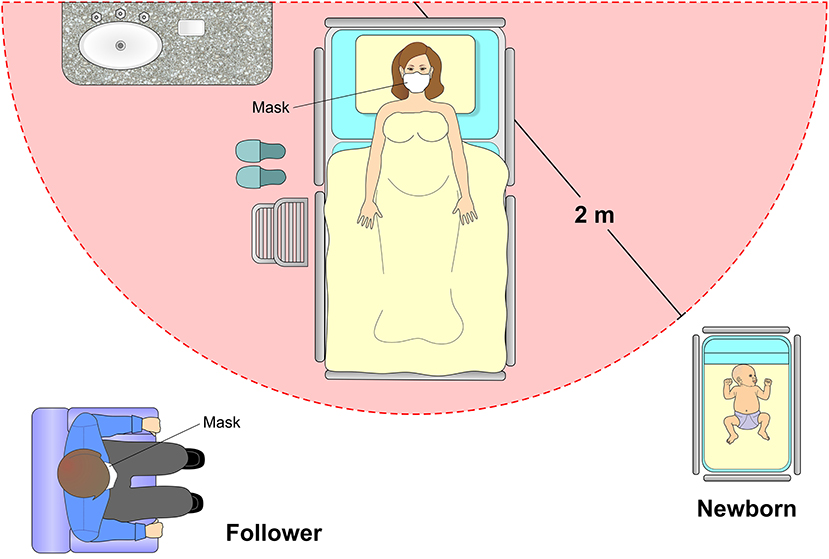
In the immediate postpartum period, a minimum distance of two meters from the cradle to the bed of the mother infected with SARS-CoV-2 is recommended. Isolation with a screen or curtains and use of masks by both parturient and companion are also advised. However, a systematic review study including 666 neonates did not show high rates of postnatal SARS-CoV-2 infection after vaginal births, breastfeeding and mother-baby interaction (65) (Figure 10).
The RT-PCR detection of SARS-CoV-2 in umbilical cord blood has not been proven to be the best target for virus detection in both vaginal and cesarean delivery. Thus, there is no reported increased risk of vertical transmission with umbilical cord clamping between 1 and 3 min after birth (64).
Breastfeeding in patients infected with SARS-CoV-2 is not contraindicated, as long as they have the desire to breastfeed and have stable clinical conditions. Factors such as severity of the symptoms, hygiene of the breasts, use of mask, and respiratory hygiene must be considered before and during breastfeeding. A study carried out by German researchers evaluated by RT-PCR the presence of the virus in milk samples from 2 infected wom
en. In the four samples collected from one of the mothers, the tests were negative for SARS-CoV-2, whereas the milk collected from the other mother had viral RNA detected for 4 days consecutively. However, the authors claim that more studies need to be carried out to determine whether the virus can be transmitted during breastfeeding (45, 66) (Figure 11).
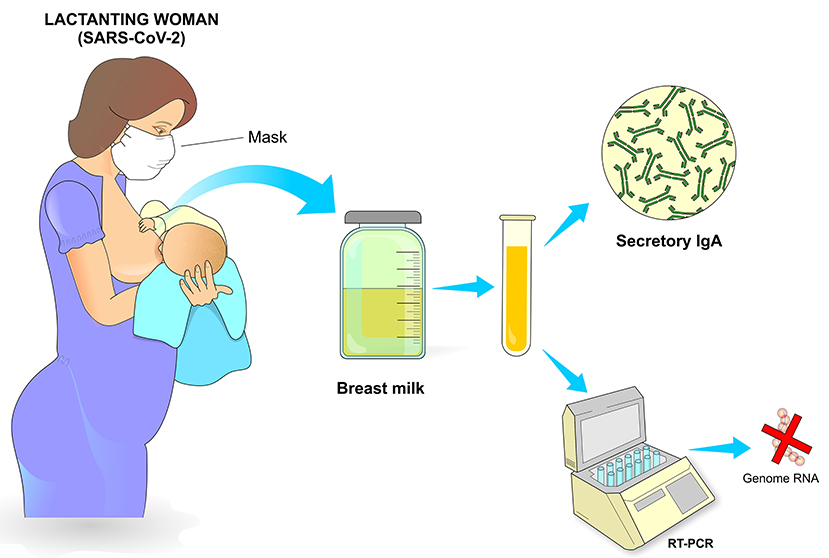
Hand and Noble state that the anti-inflammatory and anti-infective factors that are present in breastmilk becomes especially important in mitigating infectious conditions, as shown by a recent report that found a strong sIgA antibody SARS-CoV-2 immune response in breastmilk from 12 out of 15 mothers (80%) previously infected with COVID-19 (67).
Mothers infected with SARS-CoV-2 are usually asymptomatic or have mild symptoms. A prospective study investigated 70 pregnant women who had reactive PCR on admission for delivery and of these, 12 (13%) had complications in the puerperium, with 3 being admitted to intensive care unit 7 days after delivery due to hypoxia and tachypnea with signs of multifocal pneumonia and need for oxygen through nasal cannula (54).
One of the first retrospective studies conducted in China reported that between December 2019 and February 2020 nine children aged up to 1 year old were tested positive for SARS-CoV-2. Country data had just reported over 31,000 confirmed cases of Covid-19 in the same period and this study found that at least one member in the family of each child had the infection. In addition, most children had fever and mild respiratory symptoms even though more undiagnosed cases were certainly present in this population, as only hospitalized children were included in the study (68).
A prospective study also conducted in China involving 33 newborns from mothers diagnosed with Covid-19 revealed that only 3 were PCR positive for SARS-CoV-2, two were born at 40 weeks of pregnancy by cesarean sections, which were indicated due to fetal distress and severity of maternal pneumonia. After collection of nasal and rectal swabs, both newborns had the infection confirmed on the second day after birth and presented fever, lethargy and radiological signs of pneumonia.
The third child was born by cesarean section at 31 weeks after acute fetal distress and had to be resuscitated. Finally, the latter presented a condition suggestive of neonatal sepsis with positive blood culture for Enterobacter and pneumonia on the chest x-ray (69).
In another prospective study, the authors compared stillbirths, birth weight, Apgar score and number of admissions to the neonatal intensive care unit among newborns from infected (n = 69) and non-infected (n = 599) women. The results showed no significant difference between these groups with only 1 stillbirth at 37 weeks of gestation from an infected mother with decompensated diabetes (54).
In New York, an observational study conducted in 3 hospitals identified 120 neonates born from 116 mothers positive for SARS-CoV-2. All neonates were tested at 24 h of life and none were positive. Eighty-two neonates completed follow-up at day 5–7 of life. All mothers were allowed to breastfeed and 79 of 82 neonates repeated PCR test at 5–7 days of life with negative results in all of them. After 14 days of life, 72 (88%) neonates were also tested and none were positive. None of the neonates had symptoms of COVID-19 (70).
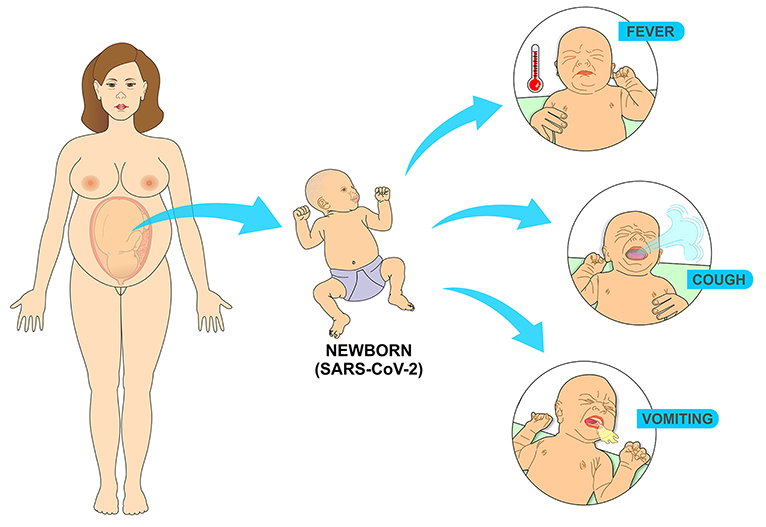
Literature review investigated the clinical characteristics of 25 neonates with positive RT-PCR in the first 28 days of life. The newborns had an average gestational age of 37 weeks and 4 days and an average birth weight of 3,041 grams. The most common signs and symptoms were fever, vomiting and cough, there were no deaths and the average hospital stay was 15 days, ranging from 5 to 40 days (71) (Figure 12).
reference link: https://www.frontiersin.org/articles/10.3389/fgwh.2021.602572/full
More information: Gee, S. et al. The legacy of maternal SARS-CoV-2 infection on the immunology of the neonate. Nat Immunol (2021). doi.org/10.1038/s41590-021-01049-2



{kind=link}