










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")


Patients who die waiting for a kidney, or who are removed from the transplant waitlist for poor health, are usually considered unfortunate victims of the ever-growing shortage of available organs.
Yet a new study has found that most candidates have had multiple opportunities to receive a transplant, but the offered organs were declined by their transplant team and subsequently transplanted in someone lower on the waitlist.
Among the candidates who received at least one offer during the study period, nearly one-third (approximately 10,000 people per year) died or were removed from the list without receiving a transplant.
Candidates who died without a transplant received a median of 16 offers (over 651 days) while waitlisted.
“Presumably, these offers were declined primarily because centers were expecting patients to get a better offer in a timely manner,” says study leader Sumit Mohan, MD, associate professor of medicine at Columbia University Vagelos College of Physicians and Surgeons and of epidemiology at the Mailman School of Public Health.
“In some cases, a decline may have been the right decision, but our data suggest that many others probably would have been better served if their transplant center had accepted one of the offers.”
76% of candidates receive at least one offer
With colleagues from Columbia University Irving Medical Center and Emory University, Mohan examined all 14 million kidney offers made between 2008 and 2015 to more than 350,000 waitlisted patients in the United States.
The data came from the United Network for Organ Sharing.
The analysis revealed that most waitlisted patients – 76% – received at least one viable offer of a kidney.
Kidney offers that were automatically declined due to a center’s minimum acceptance criteria were counted as viable offers, but offers of kidneys that were eventually discarded and never transplanted were not.
Each year, thousands receive multiple offers, but no transplant
Of the 280,041 patients who received at least one offer, 30% (approximately 85,000 people) either died on the waitlist or were removed from the waitlist before receiving a kidney.
For candidates who received at least one offer but died without a transplant, the first offer arrived a median of just 78 days after a candidate joined the list.
The vast majority of organs, 84%, were declined at least once, including organs that appeared to be an ideal immunological match.
Concern about organ quality was the reason most often provided by the transplant team for declining the kidney.
“But clearly these organs were transplantable, because all of them were eventually transplanted,” Mohan says.
“We know 93% of transplanted kidneys are still working after one year and 75% are still working after five years, which calls into question the validity of these decisions to decline offers of a kidney.”
Patients unaware of declined offers
For the most part, Mohan says, patients are unaware of declined offers.
The transplant team has just 60 minutes to accept or decline an organ offer, and often patients are not told when an organ is declined on their behalf, even after the fact.
“While the time constraints preclude real time shared decision-making, making patients aware of these organ offers subsequently will potentially improve patient engagement resulting in a process that prioritizes stated patient preference of shorter time to transplant,” Mohan says.
“It’s better to get a less-than-perfect kidney sooner than to wait years for the perfect kidney to come along. Better communication between patients and transplant centers may prompt a reconsideration of how and when to decline offers.”
Executive order
“The vast majority of kidneys are not going to the first matched candidate on the list,” Mohan says.
“The current system, which allows centers to decline offers without patient involvement or awareness, appears to make an otherwise objective allocation system more subjective than intended.”
The recent executive order directing the Secretary of Health and Human Services to improve the allocation and utilization of deceased-donor kidneys may create an opportunity for change.
The study, “Association of declining deceased donor kidney offers and outcomes in kidney transplant candidates,” was published Aug. 30 in JAMA Network Open.
A living-donor transplant is a surgical procedure to remove an organ or portion of an organ from a living person and place it in another person whose organ is no longer functioning properly.
The popularity of living-organ donation has increased dramatically in recent years as an alternative to deceased-organ donation due to the growing need for organs for transplantation and shortage of available deceased-donor organs. More than 6,000 living-organ donations are reported each year in the United States.
Living-kidney donation is the most common type of living-donor transplant. Individuals can donate one of their two kidneys, and the remaining kidney is able to perform the necessary functions. Living donors can also donate a portion of their liver, and the remaining liver regenerates, grows back to nearly its original size and performs its normal function.
Kidney and liver transplants are the most common types of living-donor organ procedures, but living people may also donate tissues for transplantation, such as skin, bone marrow and blood-forming cells (stem cells) that have been damaged or destroyed by disease, drugs or radiation.
Living-organ donation types
There are two types of living-organ donation.
Directed donation
This is the most common type of living-donor organ donation. In this type of living-donor organ donation, the donor directs the organ to a specific recipient for transplant.
The donor may be:
- A first-degree relative, such as a parent, brother, sister or adult child
- Other biologically related relatives such as uncles, aunts or cousins
- A biologically-unrelated person who has a connection with the transplant candidate, such as a spouse or significant other, a friend, or a co-worker
- A person who has heard about the transplant candidate’s need
Nondirected donation
In nondirected living-donor organ donation, also known as good Samaritan or altruistic donation, the donor does not name the recipient of the donated organ. The match is based on medical need and blood type compatibility.
In some cases, the donor may choose not to know the organ recipient. In other cases, the donor and recipient may meet if both agree and if the transplant center policy allows it.
Paired donation and donation chains

In paired-organ donation, living donors and their recipients aren’t compatible for a transplant. However, the donor of each pair is compatible with the recipient of the other pair. If both donors and recipients are willing, doctors may consider a paired donation.
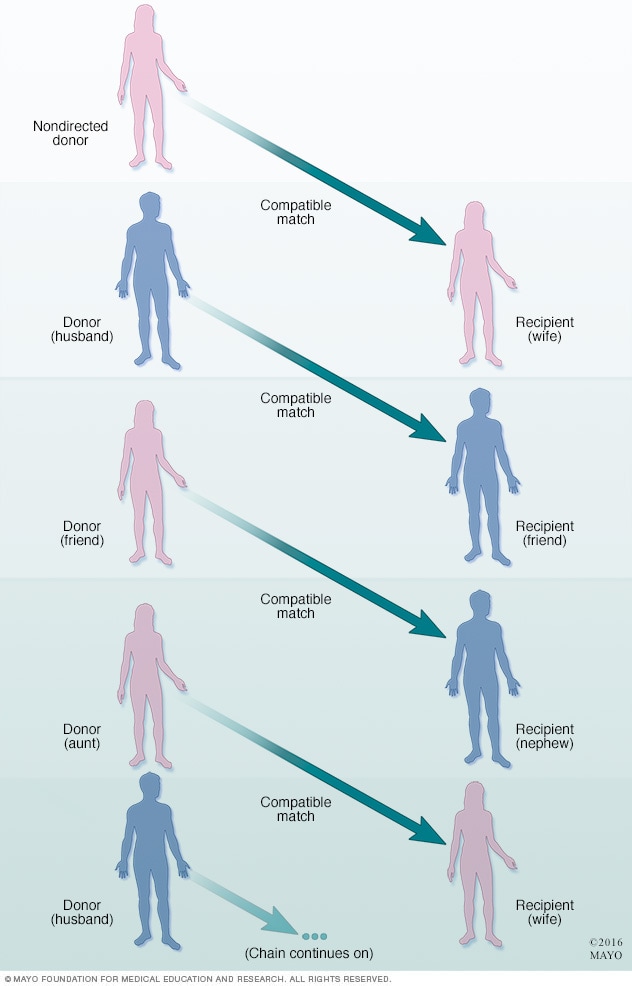
More than one pair of incompatible living donors and recipients may be linked with a nondirected living donor to form a donation chain in order to receive compatible organs.
Living donors often play an important role in paired donation and donation chains. Paired-organ donation (also known as paired exchange) may be an option when a donor and intended recipient have incompatible blood types, or when the recipient has certain antibodies that will react to the donor’s cells, causing the transplant to fail.
In paired donation, two or more organ-recipient pairs trade donors so that each recipient gets an organ that is compatible with his or her blood type. A nondirected living donor also may participate in paired-organ donation to help match incompatible pairs.
More than one pair of incompatible living donors and recipients may be linked with a nondirected living donor to form a donation chain in order to receive compatible organs. In this scenario, multiple recipients benefit from a single nondirected living donor.
Types
- Living-donor kidney transplant
- Nondirected living-donor transplant
Why it’s done
Living-donor transplantation offers an alternative to waiting for a deceased-donor organ to become available for people in need of an organ transplant.
In addition, living-donor organ transplants are associated with fewer complications than deceased-donor transplants and, overall, a longer survival of the donor organ.
Risks
The risks associated with living-donor organ donation include both short- and long-term health risks of the surgical procedure, organ function, and psychological problems following organ donation.
For the organ recipient, the risk of transplant surgery is usually low because it is a potentially lifesaving procedure. But donating an organ can expose a healthy person to the risk of and recovery from unnecessary major surgery.
Immediate, surgery-related risks of organ donation include pain, infection, hernia, bleeding, blood clots, wound complications and, in rare cases, death.
Long-term follow-up information on living-organ donors is limited, and studies are ongoing. Overall, available data shows organ donors fare very well over the long term.
Donating an organ may also cause mental health issues, such as symptoms of anxiety and depression. The donated organ may fail in the recipient and cause feelings of regret, anger or resentment in the donor.
The known health risks associated with living-organ donation vary according to the type of donation. To minimize risks, you’ll need to have extensive testing to ensure you’re eligible to donate.
Kidney donation risks
Living-donor kidney transplant is the most widely studied type of living-organ donation with more than 50 years of follow-up information. Overall, studies show the life expectancy for those who have donated a kidney is the same as for similarly matched people who haven’t.
Some studies suggest living kidney donors may have a slightly higher risk of kidney failure in the future. But this risk is still smaller than the average risk of kidney failure in the general population. Specific long-term complications associated with living-kidney donation include high blood pressure, elevated protein levels in urine and reduced kidney function.
Liver donation risks
The risks of living-liver donation also are low, but experience with this procedure is more limited because it was introduced into medical practice more recently than kidney donation. The first living-donor liver transplant was performed in 1989.
As with any surgical procedure, living-liver donation may involve surgical complications, such as infection, bleeding, blood clots and, in rare cases, death.
Living-liver donation may also cause bile leakage, narrowing of the bile duct, intra-abdominal bleeding and, in rare cases, inadequate growth of the remaining part of the liver.
More information:JAMA Network Open (2019). DOI: 10.1001/jamanetworkopen.2019.10312
Journal information: JAMA Network Open
Provided by Columbia University Irving Medical Center



{kind=link}