










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Doctors in France have described what they said was the first confirmed case of a newborn infected in the womb with COVID-19 by the mother.
The baby boy, born in March, suffered brain swelling and neurological symptoms linked to COVID-19 in adults, but has since recovered, they reported Tuesday in the journal Nature Communications.
Earlier research had pointed to the likely transmission of the virus from mother to foetus, but the study offers the first solid evidence, said senior author Daniele De Luca, a doctor at Antoine Beclere Hospital near Paris.
“We have shown that the transmission from the mother to the foetus across the placenta is possible during the last weeks of pregnancy,” he said.
Last week, researchers in Italy said that data on 31 pregnant women hospitalised with COVID-19 “strongly suggested” that the virus could be passed on to unborn infants.
A JAMA study in March reporting on a similar number of pregnant COVID-19 patients came to a similar conclusion.
But evidence remained circumstantial.
“You need to analyse maternal blood, amniotic fluid, the newborn’s blood, the placenta, et cetera,” De Luca said by phone.
“Getting all of these samples during a pandemic with emergencies everywhere has not been easy. This is why it has been suspected but never demonstrated.”
De Luca and his team pulled together this data for the case of a pregnant woman in her twenties admitted to his hospital in early March.
Because the baby was delivered by caesarean section, all of the potential sources and reservoirs of the virus remained intact.
The concentration of SARS-CoV-2, the technical name given to the virus, was highest in the placenta, the researchers found.
“From there it passed through the umbilical cord to the baby, where it develops,” De Luca said. “That is the pathway of transmission.”
‘Bad news’
The baby began to develop severe symptoms 24 hours after birth, including severe rigidity of the body, damage to white matter in the brain, and extreme irritability.
But before doctors could settle on a course of treatment, the symptoms began to recede. Within three weeks, the newborn had almost fully recovered on his own.
Three months later, his mother is without symptoms.
“The bad news is that this actually happened, and can happen,” De Luca said. “The good news is that it is rare – very rare compared to the global population.”
Among the thousands of babies born to mothers with COVID-19, no more than one or two percent have tested positive for the virus, and even fewer show serious symptoms, said Marian Knight, a professor of maternal and child population health at the University of Oxford who was not involved in the research.
“The most important message for pregnant women remains to avoid infection through paying attention to hand washing and social distancing measures,” she said.
Others said the case study shed light on how the virus passes from mother to child.
“This report adds knowledge to a possible mechanism of transfer to the baby, via the placenta,” commented Andrew Shennan, a professor of obstetrics at King’s College London.
“But women can remain reassured that pregnancy is not a significant risk factor for them or their babies with COVID-19.”
Discussion
We report a proven case of transplacental transmission of SARS-CoV-2 from a pregnant woman affected by COVID-19 during late pregnancy to her offspring. Other cases of potential perinatal transmission have recently been described, but presented several unaddressed issues.
For instance, some failed to detect SARS-CoV-2 in neonates or only reported the presence of specific antibodies1,2,4; others found the virus in the newborn samples but the transmission route was not clear as placenta, amniotic fluid and maternal or newborn blood were not systematically tested in every mother-infant pair3,5,6,11,12.
A classification for the case definition of SARS-CoV-2 infection in pregnant women, fetuses and neonates has recently been released and we suggest to follow it to characterize cases of potential perinatal SARS-CoV-2 transmission.
According to this classification system, a neonatal congenital infection is considered proven if the virus is detected in the amniotic fluid collected prior to the rupture of membranes or in blood drawn early in life, so our case fully qualifies as congenitally transmitted SARS-CoV-2 infection, while the aforementioned cases would be classified as only possible or even unlikely13.
Another recent report describes a case with similar placental findings, but it has been classified only as probable case of congenital SARS-CoV-2 infection, because cord and newborn blood could have not been tested14.
Both “E” and “S” gene of SARS-CoV-2 were found in each and every specimen, thus they were considered all positive, according to the European Centre for Disease Control recommendations (https://www.ecdc.europa.eu/en/all-topics-z/coronavirus/threats-and-outbreaks/covid-19/laboratory-support/questions).
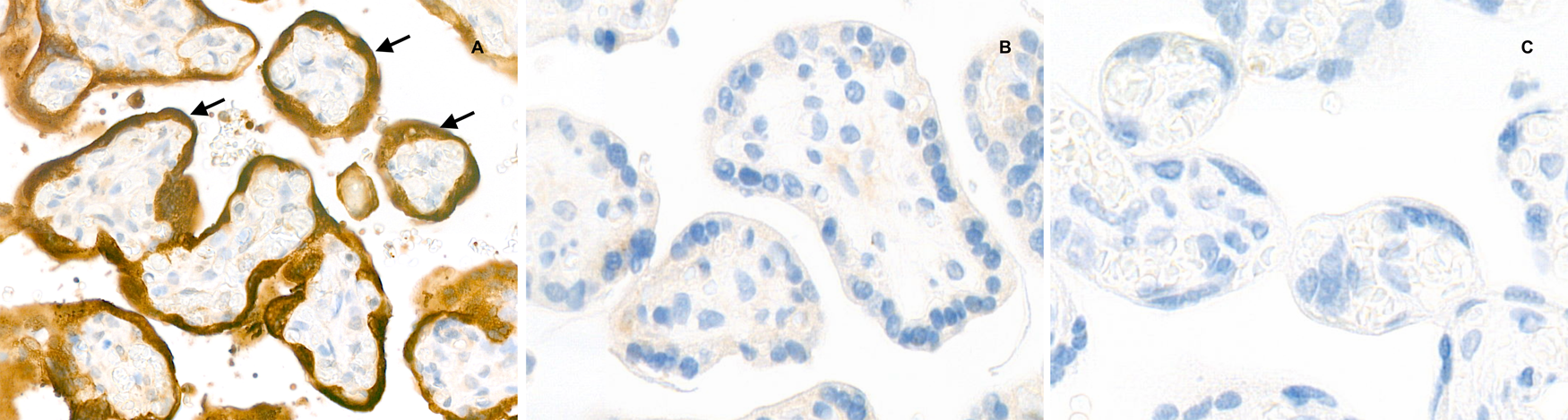
Of note, the viral load is much higher in the placental tissue than in amniotic fluid or maternal blood: this suggests the presence of the virus in placental cells, which is consistent with findings of inflammation seen at the histological examination.
Finally, the RT-PCR curves of neonatal nasopharyngeal swabs at 3 and 18 day of life are higher than that at the first day (while the baby was in full isolation in a negative pressure room): this is also another confirmation that we observed an actual neonatal infection, rather than a contamination.
Thus, these findings suggest that:
(1) maternal viremia occurred and the virus reached the placenta as demonstrated by immunohistochemistry;
(2) the virus is causing a significant inflammatory reaction as demonstrated by the very high viral load, the histological examination and the immunohistochemistry;
(3) neonatal viremia occurred following placental infection. Our findings are also consistent with a case study describing the presence of virions in placental tissue, although this did not report neither placental inflammation, nor fetal/neonatal infection15.
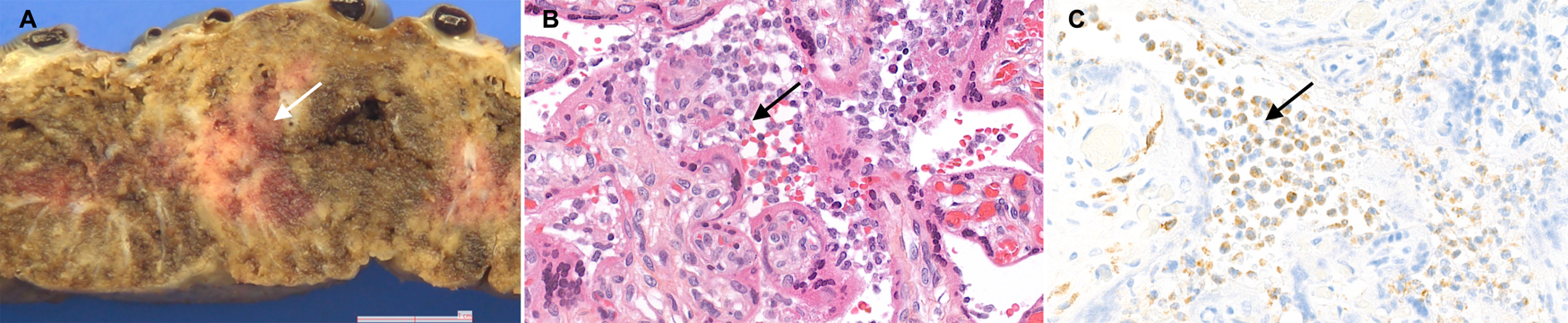
The placenta showed signs of acute and chronic intervillous inflammation consistent with the severe systemic maternal inflammatory status triggered by SARS-CoV-2 infection. As RT-PCR on the placental tissue was positive for SARS-CoV-2, and both maternal and neonatal blood samples were also positive, the transmission clearly occurred through the placenta.
Interestingly, placentas from women affected by SARS-CoV-1 presented similar pathological findings of intervillositis, with intervillous fibrin deposition16. Angiotensin-converting enzyme 2 (ACE2) is known to be the receptor of SARS-CoV-2 and is highly expressed in placental tissues17.
Animal data show that ACE2 expression changes in fetal/neonatal tissues over time and reaches a peak between the end of gestation and the first days of postnatal life17.
The combination of these data and our findings confirms that transplacental transmission is indeed possible in the last weeks of pregnancy, although we cannot exclude a possible transmission and fetal consequences earlier during the pregnancy, as there are no definite literature data available yet.
Interestingly, we described a case of congenital infection associated with neurological manifestations following neonatal viremia. Suspected neonatal SARS-CoV-2 infections presented with non-specific symptoms4 or pneumonia3, while neurological symptoms are commonly observed in adult patients, especially due to the inflammatory response18,19.
Early neurological manifestations were also observed in another neonate born to SARS-CoV-2 positive mother, although vertical transmission was not fully investigated12. Conversely, after the viremia, our case clearly presented neurological symptoms and inflammatory findings in CSF.
There was no other viral or bacterial infection and all other neonatal disorders potentially causing these clinical manifestations were excluded. Neuroimaging consistently indicated white matter injury, which can be caused by the vascular inflammation induced by SARS-CoV-2 infection, as similar images have been anecdotally found in adult patients20,21.
In conclusion, we have demonstrated that the transplacental transmission of SARS-CoV-2 infection is possible during the last weeks of pregnancy. Transplacental transmission may cause placental inflammation and neonatal viremia. Neurological symptoms due to cerebral vasculitis may also be associated.
Journal information:Nature Communications
Cite this article
Vivanti, A.J., Vauloup-Fellous, C., Prevot, S. et al. Transplacental transmission of SARS-CoV-2 infection. Nat Commun 11, 3572 (2020). https://doi.org/10.1038/s41467-020-17436-6



{kind=link}