









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



SARS-CoV-2 infections are a worldwide pandemic, posing a se- vere risk to health [1]. Human coronavirus, SARS-CoV-2, is highly pathogenic with severe pneumonia associated with rapid virus replica- tion.
Arising in Wuhan China December 2019, the current COVID-19 epidemic has rapidly grown with person-to-person infection expanding to become a global health emergency now on pandemic scale [2].
Since there are no currently accepted therapies for corona virus disease 2019 worldwide search for treatment options are ongoing.
Past experiences with viral infections are important in this respect, like in Argentina practicedby Dr. Julio Maiztegui [3].
Convalescent plasma therapy and mesenchymal stem cell therapy are two of potential options for Covid-19, mentioned, in case series and non- randomized studies from different countries [4].
On the other hand, Glucocorticoids like Dexamethasone, may modulate inflammation- mediated lung injury and thereby reduce progression to respiratory failure and death [5].

The triple strategy that has shown individually, safe and possible effectiveness in the treatment for Covid-19 pneumonia, could be a way of synergic treatment, following this review.
Mesenchymal stem cell therapy
Mesenchymal stem cell (MSC) therapy has been the subject of research in many different fields of medicine due to its immunomodulatory and reparative effects.
The alveolar injury by COVID-19 is characterized by the impairment of endothelial and type I alveolar cell (pneumocyte) barrier, which eventually results in an intense accumulation of proteinaceous fluid (alveolar edema) and mononuclear cell (lymphocytes) infiltrates in interalveolar septa.
Extravasated and/or resident MSCs can trigger a series of direct and indirect repairing mechanisms. Clearance of the increased alveolar edema can be induced by the release of KGF by enhancing sodium-dependent alveolar fluid clearance through type II alveolar sodium channels.
The MSC-released TSG6 decreases neutrophil functions, which directly affects improvement of the vascular endothelial and alveolar epithelial barriers [6].
The resolution of inflammation can be further enhanced by the increased release of IL-10 and decreased release of TNF-a, which are mediated by LXA4 and PGE2. Increased epithelial repair in type II alveolar cells can be restored by the release of Ang1.
MSCs can also facilitate the phagocytosis of bacteria by the intra-alveolar and interalveolar macrophages by releasing the antimicrobial peptide LL- 37 or by the transfer of extracellular vesicles to macrophages from MSCs [6].
Additionally, MSCs can exert their actions through mitochondrial transfer to injured alveolar cells, thus increasing their ATP content, which would improve bioenergetics and increase alveolar epithelial function, improving surfactant release by type II alveolar cells.
MSCs can degrade or inhibit ARDS-induced fibrotic tissue formation (collagen fiber accumulation) to modulate the extracellular matrix by releasing MMPs and TIMPs.
In MSC-based therapies, infusion of auto/allogeneic MSCs is applied through two primary routes (intravenous and intratracheal/intrabronchial) [7].
The most important mechanism is that MSCs release many paracrine factors, such as micro-RNA, interacting with the immune response to exert immunoregulation and anti-inflammatory effects [8].
Three publications, two from China, one case report and one case series, and one from Spain, have reported positive results of intravenous administration of Umbilical Cord-MSC (UC-MSC) or Adipose Derived-MSC (AD-MSC) in severely ill COVID-19 patients [9,10].
It has been reported that, clinical, radiological, and laboratory improvement has been observed within days of therapy in these patients [8-10]. Up to date, there are more than 50 trialsregistered on going with MSC for Covid-19 (10) (56 clinical trials were registered in clinicaltrials.gov under COVID and “mesenchymal” terms as of the writing date of this review).
Treatment with intravenous administration of AD-MSC or UC- MSC in severe COVID-19 pneumonia under mechanical ventilation in a small case series did not induce significant adverse events and was followed by clinical and biological improvement in most subjects [8-10].
It is considered that infection of mesenchymal stem cells with SARS-CoV-10 is not an expected condition since they lack ACE2 receptors [11-13]. As well, ongoing cytokine production stimulate these cells to produce anti-inflammatory and trophic mediators, which help to confine the cytokine storm and the resulting lung injury.
The remarkable new data using MSC demonstrate successful harnessing of natural endogenous pathways with powerful protective properties [2].
The dose recommended in the BALMYS-19-“BAttLe against COvid using MesenchYmal Stromal cells” was 1.000.000 MSC X kg [10].
Dexamethasone
In patients hospitalized with Covid-19, the preliminary results of the controlled, open-label Randomized Evaluation of Covid-19 Therapy (RECOVERY) trial of dexamethasone showed that the use of it resulted in lower 28-day mortality among those who were receiving either invasive mechanical ventilation or oxygen alone at randomization but not among those receiving no respiratory support [5].
The benefit was also clear in patients who were being treated more than 7 days after symptom onset, when inflammatory lung damage is likely to have been more common [5].
The protocol combines the methods that were used in large, simple trials of treatments for acute myocardial infarction in the 1980s with the opportunities provided by digital health care in the 2020s [14-16].
The RECOVERY trial provides evidence that treatment with dexamethasone at a dose of 6 mg once daily for up to 10 days reduces 28-day mortality in patients with Covid-19 who are receiving respiratory support [5].
Dexamethasone is on the list of essential medicines of the World Health Organization and is readily available worldwide at low cost. Guidelines issued by the U.K. chief medical officers and by the National Institutes of Health in the United States have already been updated to recommend the use of glucocorticoids in patients hospitalized with Covid-19 [17,18].
Slower clearance of viral RNA has been observed in patients with SARS, MERS, and influenza who were treated with systemic glucocorticoids, but the clinical significance of these findings is unknown.
Unlike with SARS, in which viral replication peaks in the second week of illness, viral shedding in SARS-CoV-2 appears to be higher early in the illness and de- clines thereafter [18].
Convalescent plasma
One of the potential treatment options that is being evaluated extensively is convalescent plasma therapy, which provides passive immunization. With convalescent plasma therapy, viral neutralization and consequently decreased target organ injury is aimed.
The rationale behind this treatment is basic knowledge and experience from the recent studies on MERS, SARS and H1N1 infections and several other infections at the beginning of twentieth century [20].
In Argentina it was used for the treatment of the Argentine hemorrhagic fever with very good results to reduce mortality [3] a few years ago by Dr. Julio Maiztegui.
Patients who want to donate for convalescent plasma must have recovered from COVID-19 symptoms, their SARS-CoV-2 PCR tests should have become negative, and they must have adequate antibody response to SARS-CoV-2. It is considered to be most effective during the initial week, and it may be considered to be ineffective after 14th day [21-23].
Prior to administration presence of IgA deficiency or known allergy to contents (i.e. citrate) of the product should be ruled out. Presence of IgA deficiency may result in severe anaphylactic reaction [20].
Evidence shows that convalescent plasma from patients who have recovered from viral infections can be used as a treatment without the occurrence of severe adverse events. Therefore, it might be worthwhile to test the safety and efficacy of convalescent plasma transfusion in SARS-CoV-2-infected patients [22].
The doses of Convalescent Plasma used as described by the different studies are varied. A Chinese pilot study showed a minimal use of a single dose of 200 mL convalescent plasma with neutralizing antibody titers >1:640.
Another study by Bin Zhang et al., reported a maximum of 2400 mL of convalescent plasma administered to a 73 years old male patient [23].
The dose we recommend of Convalescent Plasma is 300 mL/ unique dose.
The Argentinian Protocol. Triple Treatment Strategy as Immunomodulatory and Antiviral Effect for Covid-19
Although it has been observed from one case that intravenous infusion of plasma and mesenchymal stem cells have a synergistic therapeutic effect on patients with severe COVID-19 pneumonia [8], in theory, the mechanisms of action of convalescent plasma and mesenchymal stem cells have complementary characteristics.
We believe that a triple treatment strategy, including dexamethasone, might benefit patients with COVID-19 pneumonia without better options to stop the cytokine storm.
Eligibility for MSC + Convalescent Plasma + Dexamethasone as a Triple Treatment Strategy on a Same Day
Inclusion criteria
- Patient 18 years old or older.
- Hospitalized with highly severe COVID-19 respiratory symp- toms and confirmation of infectionpositive using the RT-PCR test COVID-19 SARS-CoV-2 (real-time PCR).
- Patient duly informed, to the extent of their conditions, who is a voluntary signer of a comprehensive Informed Consent Form. In case of not being able to do so, the authorizing signature of the legal representative, the support, the spouse, the cohabitant, the relative or the close friend will be obtained.
- Severely compromised patient, presenting any of these symptoms and / or parameters:
- Dyspnea
- Respiratory rate => 30 I min
- Blood oxygen saturation <= 93%
- Ratio between partial pressure of arterial oxygen and fraction of inspired oxygen <300
- Lung infiltrates> 50% within 24 to 48 hours
Or that it is in a terminal state and for whom the doctor considers that it has a high-riskmortality
- Respiratory failure
- Septic shock
- Multiple organ failure or dysfunction
Exclusion criteria
- Contraindication to transfusion: history of anaphylaxis to blood products.
- In relation to other comorbidities: according to the criteria of the treating physician.
Conclusion
Based on evidence reported in systematic reviews, meta-analysis and clinical trials including systemic applied MSC, Convalescent
Plasma and Dexamethasone, this triple theoretical therapy strategy appears to be safe in different conditions and situations and could prove a useful way for COVID-19 patients given their immunomod- ulatory and anti-inflammatory properties.
This theoretical treatment stimulates our group to design a Phase 1 protocol for the treatment of severe pneumonia for Covid-19 in Argentina.
Acknowledgements
We thank Dr Marcelo A. Fernandez Vina for his helpful comments and invaluable insights that contributed to the development of this treatment protocol.
Declarations
MFV, LC, MIS, RFV, have nothing to declare related to this manuscript.
Funding Information
This work was funded by Fundación Don Roberto Fernández Viña.
COVID-19 – Mesenchymal Stem Cells
Are Stem Cells a Solution to COVID-19 Crisis?
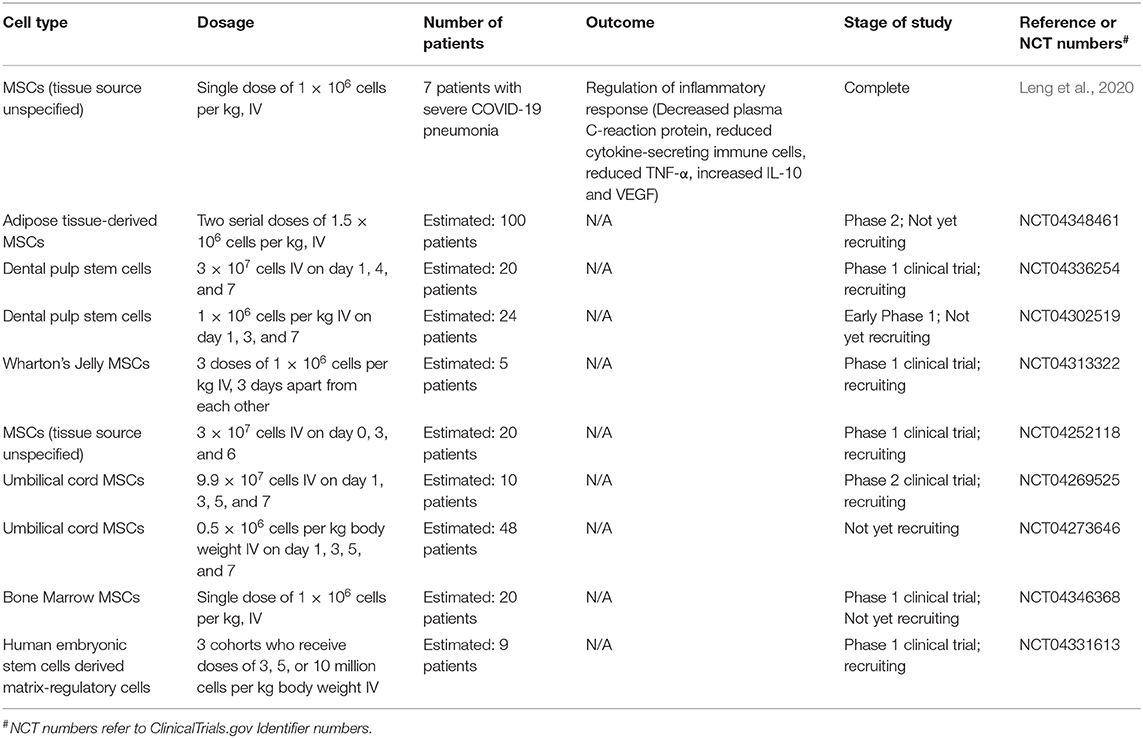
MSCs could be the most promising candidate for the treatment of SARS-CoV-2 infections (Table 1). Since the key for the treatment of SARS-CoV-2 infection lies in the management of the cytokine storm in the lungs, MSCs are well-suited considering their main mechanism of action is through their immunomodulatory and anti-inflammatory properties (Fatima et al., 2017).
The safety profile and efficacy of MSCs are well-established based on the results from a number of completed clinical studies investigating the therapeutic potential of these therapies in lung diseases such as ARDS (Matthay et al., 2019; Chen J. et al., 2020) and bronchopulmonary dysplasia (Namba, 2019), cardiovascular diseases (Kim et al., 2015; Suvakov et al., 2020), diabetes (Thakkar et al., 2015; Cho et al., 2018), and spinal cord injury (Xu and Yang, 2019).
Other types of stem cells investigated for potential treatment of SARS-CoV-2 infections include genetically engineered human induced pluripotent stem cells (iPSC). A recent study presented a deleterious effect on the cells in vitro when iPSCs were exposed to SARS-CoV-2, where the pluripotency of iPSCs was lost leading to fibroblast-like phenotype (Zebin et al., 2020). Therefore, evidence-based selection of stem cell type for the treatment of COVID-19 is critical for safety and efficacy.
Factors Affecting the Quality of MSC
The successful translation of MSC-based therapies into the clinic for treatment of COVID-19-induced lung injuries is dependent on a number of factors. In addition to desirable therapeutic effects, it is also important to understand the mechanism of action and the influence of various in vivo environments on the integrity of these cells.
Stem cells can be environmentally preconditioned by certain stimuli such as hypoxia or ischemia, which can induce certain signaling pathways to improve engraftment, survival, and function of transplanted cells in harsh environments within the injured lung (Sart et al., 2014; Kim et al., 2015; Saparov et al., 2016).
Other methods of preconditioning stem cells include the formation of three-dimensional stem cell aggregates that lead to enhanced extracellular matrix secretion, anti-inflammatory properties and cell survival (Bartosh et al., 2010; Sart et al., 2014). Pre-treatment of MSCs with various pharmacological factors can, in fact, improve therapeutic effects and tissue repair capabilities (Hu and Li, 2018).
Furthermore, bioengineering approaches such as the use of bioreactors can overcome the limitations of a large scale production of stem cells necessary for transplantation and maintenance of the stemness during and after delivery to patients (Madl et al., 2018).
Therefore, these technologies can accelerate the transition from bench to bedside without compromising the quality of the stem cells reaching patients. For example, tuneable materials can be used as an artificial niche to expand or differentiate stem cells to mature cell types (Yang et al., 2014; Madl et al., 2017).
Materials such as hydrogels used as carriers for stem cells can also lead to enhanced regenerative response by regulating fate and activity of transplanted stem cells (Engler et al., 2006; Chaudhuri et al., 2016). These approaches are currently less widely used for pulmonary applications compared to other target organs and thus future investigations will lead to innovative solutions.
Is the Treatment Efficacy Dependent on the Delivery Route?
In the majority of clinical trials investigating the treatment of SARS-CoV-2 infections so far, MSCs are delivered via the intravenous route. Since intravenous route does not specifically target lungs, the inhalation route that delivers cells directly to lungs could be more effective.
However, uniform delivery of cells to lungs through inhalation is technically challenging (Kim et al., 2016; Kim and Chrzanowski, 2019). Strong evidence is emerging to suggest that the therapeutic potential of MSCs is attributed mostly to their secreted EVs via paracrine effects, and MSCs could also be referred to as medicinal signaling cells (Bjørge et al., 2018; Kim et al., 2019).
Delivery of EVs to lungs is feasible and exogenous EVs can facilitate prompt activity directly at the injured site. There is a pilot clinical study that intends to deliver MSC-derived exosomes via the inhalation route to patients with severe pneumonia arising from SARS-CoV-2 infection (NCT04276987).
In this clinical trial, the main advantage of administering MSC-derived exosomes via inhalation route compared to the intravenous administration is the prevention of their aggregation within the injured microcirculation.
In addition, MSC-derived exosomes have other advantages over MSCs including lower or no risk of mutagenicity and oncogenicity as well as the storage stability of several weeks or months facilitating less urgent transportation and administration.
A recent study using animal models of pulmonary fibrosis also demonstrated therapeutic potential of inhaled lung spheroid cell-secretome and exosomes for lung regeneration (Dinh et al., 2020).
While the intravenous route is the most widely used often for the ease of administration albeit invasive, the route of cell delivery should be tailored according to the disease in question and patient’s circumstances (Kim and Chrzanowski, 2019).
As evident from a number of clinically available inhaled medications for chronic lung disease, the inhalation route of delivering therapeutics to the lungs is a more direct route with lower incidence of adverse effects, compared to the intravenous route. Nevertheless, the environment in the hospital has to be appropriately managed for inhaled administration of a treatment in COVID-19 patients. A
number of studies have demonstrated the feasibility of delivering stem cells via spray for direct pulmonary delivery with high viability (Kardia et al., 2016; Kim et al., 2016; Skolasinski et al., 2020). Inhalation route of stem cell administration is an opportunity for efficient delivery of stem cells directly to the lungs, yet it remains an under-explored research area in the field.
Rationale for Recommendation
MSCs are investigational products that have been studied extensively for broad clinical applications in regenerative medicine (31) and for their immunomodulatory properties.32 No MSCs are approved by the Food and Drug Administration (FDA) for the treatment of COVID-19. There are insufficient data to assess use of MSCs for the treatment of COVID-19.
The FDA has recently issued several warnings about patients being potentially vulnerable to stem cell treatments that are illegal and potentially harmful.33 Several cord blood-derived products are currently licensed by the FDA for indications such as the treatment of cancer (e.g., stem cell transplant) or rare genetic diseases, and as scaffolding for cartilage defects and wound beds.
None of these products are approved for the treatment of COVID-19 or any other viral disease.34 In the United States, MSCs should not be used for the treatment of COVID-19 outside of an FDA-approved clinical trial, expanded access programs, or an Emergency Investigational New Drug application (AII).
Rationale for Use in COVID-19
MSCs are multipotent adult stem cells that are present in most human tissues, including the umbilical cord. MSCs can self-renew by dividing and can differentiate into multiple types of tissues, including osteoblasts, chondroblasts, adipocytes, hepatocytes, and others, which has led to a robust clinical research agenda in regenerative medicine.
It is hypothesized that MSCs could reduce the acute lung injury and inhibit the cell-mediated inflammatory response induced by severe acute respiratory syndrome coronavirus 2 (SARS-COV-2).
Furthermore, MSCs lack the angiotensin-converting enzyme 2 receptor that SARS-COV-2 uses for viral entry into cells; therefore, MSCs are resistant to infection.35,36
Clinical Data
Data supporting the use of MSCs in patients with viral infections, including COVID-19, are limited to case reports and small, open-label studies.
Clinical Data for COVID-19
- A pilot study of intravenous MSC transplantation in China enrolled 10 patients with confirmed COVID-19 categorized according to the National Health Commission of China criteria as critical, severe, or common type. Seven patients (one with critical illness, four with severe illness, and two with common-type illness) received MSCs; three patients with severe illness received placebo. All seven patients who received MSCs recovered. Among the three severely ill control patients, one died, one developed acute respiratory distress syndrome (ARDS), and one remained stable with severe disease.37
Clinical Data for Other Viral Infections
- In an open-label study of MSCs for the treatment of H7N9 influenza in China, 17 patients received MSC treatment plus standard of care, and 44 patients received standard of care only. In the MSC group, three patients (17.6%) died; in the control group, 24 patients (54.5%) died. The 5-year follow-up was limited to five patients in the MSC group. No safety concerns were identified.38
Clinical Trials
See ClinicalTrials.gov for a list of clinical trials evaluating MSCs for the treatment of COVID-19 and COVID-19-related ARDS that are underway and recruiting participants.
Adverse Effects
Risks associated with MSC transfusion appear to be uncommon. The potential risks include failure of the cells to work as expected, potential for MSCs to multiply or change into inappropriate cell types, product contamination, growth of tumors, infections, thrombus formation, and administration site reactions.39
Considerations in Pregnancy
There are insufficient data to assess the risk of MSC use during pregnancy.
Considerations in Children
There are insufficient data on the efficacy and safety of MSC use in children.
References
- Casadevall A, Pirofski LA (2020) The convalescent sera option for con- taining COVID-19. J Clin Invest 30: 1545-1548.
- Metcalfe SM (2020) Mesenchymal stem cells and management of COVID-19 pneumonia. Med Drug Discov 5: 100019.
- Maiztegui JI (1975) Clinical and epidemiological patterns of Argentine hemorrhagic fever. Bull World Health Organ 52: 567-575.
- Valk SJ, Piechotta V, Chai KL, Doree C, Monsef I, et al. (2020) Convales- cent plasma or hyperimmune immunoglobulin for people with COVID-19: A Rapid Review. Cochrane Database Syst Rev 5: CD013600.
- Lane HC, Fauci AS (2020) Research in the Context of a Pandemic. N Engl J Med: 32678528.
- Laffey JG, Matthay MA (2017) Fifty years of research in ARDS. Cell- based therapy for acute respiratory distress syndrome. Biology and poten- tial therapeutic value. Am J Respir Crit Care Med 196: 266-273.
- Can A, Coskun H (2020) The rationale of using mesenchymal stem cells in patients with COVID-19- related acute respiratory distress syndrome: What to expect. STEM CELLS Transl Med 1-16.
- Peng H, Gong T, Huang X, Sun X, Luo H, et al. (2020) A synergistic role of convalescent plasma and mesenchymal stem cells in the treatment of se- verely ill COVID-19 patients: A clinical case report. Stem Cell Res Ther 11: 291.
- Leng Z, Zhu R, Hou W, Feng Y, Yang Y, et al. (2020) Transplantation of ACE2- mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis 11: 216-228.
- Sanchez-Guijo F, García-Arranz M, López-Parra M, Monedero P, Ma- ta-Martínez C, et al, (2020) Adipose-derived mesenchymal stromal cells for the treatment of patients with severe SARS- CoV-2 pneumonia requir- ing mechanical ventilation. A proof of concept study. E Clinical Medicine: 100454.
- Mesenchymal Stem Cells Covid-19 (2019) National Institutes of Health, USA.
- Metcalf SM (2020) Mesenchymal stem cells and management of COVID-19 pneumonia. Med Drug Discov 5: 100019.
- Atluri S, Manchikanti L, Hirsch JA (2020) Expanded umbilical cord mes- enchymal stem cells (UC-MSCs) as a therapeutic strategy in managing critically ill COVID-19 patients: The case for compassionate use. Pain Physician 23: 71-83.
- Yusuf S, Collins R, Peto R (1984) Why do we need some large, simple randomized trials? Stat Med 3: 409-422.
- ISIS-2 (Second International Study of Infarct Survival) Collaborative Group (1988) Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarc- tion: ISIS-2. Lancet 2: 349-360.
- Collins R, Bowman L, Landray M, Peto R (2020) The magic of randomiza- tion versus the myth of real-world evidence. N Engl J Med 382: 674-678.
- Whitty C (2020) Dexamethasone in the treatment of COVID-19: Imple- mentation and management of supply for treatment in hospitals. Medicines and Healthcare Products Regulatory Agency, London, UK.
- COVID-19 treatment guidelines (2020) National Institutes of Health, Bethesda, Maryland, United States.
Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexametha- sone in Hospitalized Patients with Covid-19 – Preliminary Report. N Engl J Med: 32678530.- Altintas ND (2020) Convalescent Plasma and Mesenchymal Stem Cell Therapy. J Crit Intensive Care 11: 41-42.
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395: 497-506.
- Chen L, Xiong J, Bao L, Shi Y (2020) Convalescent plasma as a potential therapy for COVID-19. Lancet Infect Dis 20: 398-400.
- Rajendran K, Krishnasamy N, Rangarajan J, Rathinam J, Natarajan M, et al. (2020) Convalescent plasma transfusion for the treatment of COVID-19: Systematic review. J Med Virol: 1-9.
- Samsonraj RM, Raghunath M, Nurcombe V, Hui JH, van Wijnen AJ, Cool SM. Concise review: multifaceted characterization of human mesenchymal stem cells for use in regenerative medicine. Stem Cells Transl Med. 2017;6(12):2173-2185. Available at: https://www.ncbi.nlm.nih.gov/pubmed/29076267.
- Li N, Hua J. Interactions between mesenchymal stem cells and the immune system. Cell Mol Life Sci. 2017;74(13):2345-2360. Available at: https://www.ncbi.nlm.nih.gov/pubmed/28214990.
- Food and Drug Administration. FDA warns about stem cell therapies. 2019. Available at: https://www.fda.gov/consumers/consumer-updates/fda-warns-about-stem-cell-therapies. Accessed July 2, 2020.
- Food and Drug Administration. Approved cellular and gene therapy products. 2019. Available at: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/approved-cellular-and-gene-therapy-products. Accessed July 2, 2020.
- Lukomska B, Stanaszek L, Zuba-Surma E, Legosz P, Sarzynska S, Drela K. Challenges and controversies in human mesenchymal stem cell therapy. Stem Cells Int. 2019:9628536. Available at: https://www.ncbi.nlm.nih.gov/pubmed/31093291.
- Shetty AK. Mesenchymal stem cell infusion shows promise for combating coronavirus (COVID-19)- induced pneumonia. Aging Dis. 2020;11(2):462-464. Available at: https://www.ncbi.nlm.nih.gov/pubmed/32257554.
- Leng Z, Zhu R, Hou W, et al. Transplantation of ACE2- mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis. 2020;11(2):216-228. Available at: https://www.ncbi.nlm.nih.gov/pubmed/32257537.
- Chen J, Hu C, Chen L, et al. Clinical study of mesenchymal stem cell treating acute respiratory distress syndrome induced by epidemic influenza A (H7N9) infection, a hint for COVID-19 treatment. Engineering (Beijing). 2020. Available at: https://www.ncbi.nlm.nih.gov/pubmed/32292627.
- Centers for Disease Control and Prevention. Stem cell and exosome products. 2019. Available at: https://www.cdc.gov/hai/outbreaks/stem-cell-products.html. Accessed July 2, 2020.



{kind=link}
[…] COVID-19: A new triple strategy could be effective for treating serious… […]