









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The Moderna COVID-19 vaccine, which the company says was recently demonstrated to have 94 percent efficacy, causes the human immune system to produce potent antibodies that endure for at least three months, a study showed Thursday.
Researchers at the National Institute for Allergies and Infectious Diseases (NIAID), which co-developed the drug, studied the immune response of 34 adult participants, young and old, from the first stage of a clinical trial.
Writing in the New England Journal of Medicine, they said that the antibodies, which stop the SARS-CoV-2 virus from invading human cells, “declined slightly over time, as expected, but they remained elevated in all participants 3 months after the booster vaccination.”
The vaccine, called mRNA-1273, is administered in two injections given 28 days apart.
Even though the number of antibodies in the study subjects faded over time, it is not necessarily a cause for concern.
NIAID director Anthony Fauci and other experts have said it is very likely that the immune system will remember the virus if re-exposed later on, and then produce new antibodies.
Encouragingly, the study showed that the vaccine activated a certain type of immune cell that should help out in the so-called memory response, but only longer term study will confirm if this will really be the case.
“Positives from the study include evidence that a relatively strong antibody response remains 90 days after the second dose of the vaccine,” said virologist Benjamin Neuman, a virologist at Texas A&M University-Texarkana.
“The amount of vaccine-produced antibodies was higher in younger patients than in older patients, but reasonably strong immune responses were still seen even in patients up to 70 years of age.”
The Moderna vaccine will be reviewed by an advisory committee of the Food and Drug Administration (FDA) on December 17, and could be green lit for emergency approval soon after.
Like another vaccine produced by Pfizer and BioNTech, it is based on a new technology that uses genetic material in the form of mRNA (messenger ribonucleic acid).
The mRNA is encased in a lipid molecule and injected into the arm, where it causes cells inside our muscles to build a surface protein of the coronavirus.
This tricks the immune system into believing it’s been infected with a microbe, and trains it to build the right kind of antibodies for when it encounters the real virus.
mbines Moderna’s mRNA (messenger RNA) delivery platform with the stabilized SARS-CoV-2 spike immunogen (S-2P) developed by NIAID scientists.
The vaccine candidate transitioned from early development with NIAID to the Biomedical Advanced Research and Development Authority (BARDA), part of the Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response, for advanced development and manufacturing support, to meet the federal government’s Operation Warp Speed(link is external) (OWS) goals.
The Phase 3 vaccine efficacy trial, known as COVE, was begun under OWS, a multi-agency collaboration led by HHS and the Department of Defense that aims to accelerate the development, manufacturing and distribution of medical countermeasures for COVID-19. The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership advised on the trial protocol design and endpoints to ensure a harmonized approach across multiple vaccine efficacy trials.
The partnership brings NIH together with other HHS agencies and government partners and representatives from academia, philanthropic organizations, and numerous biopharmaceutical companies to develop a coordinated research strategy for prioritizing and speeding development of the most promising treatments and vaccines.
More than 30,000 participants at 100 clinical research sites in the United States are participating in the study, which launched on July 27, 2020, after results from earlier stage clinical testing indicated that the vaccine candidate is well-tolerated and immunogenic. Recognizing the disproportionate impact of the epidemic on underrepresented minority populations, investigators worked with community engagement partners to enroll a diverse pool of participants. 37% of trial volunteers are from racial and ethnic minorities.
The COVE trial is sponsored by Moderna. BARDA and NIAID are providing funding and technical support for the trial. Twenty-five NIH-funded COVID-19 Prevention Network(link is external) sites enrolled participants in the trial.
As part of the arrangement under OWS, representatives from NIAID, BARDA and Moderna are part of the oversight group that receives recommendations from the trial’s independent DSMB. The same DSMB also oversees the additional OWS-supported Phase 3 clinical trials evaluating COVID-19 vaccine candidates.
The co-principal investigators for the study are Hana M. El Sahly, M.D., principal investigator of the NIAID-funded Infectious Diseases Clinical Research Consortium site at Baylor College of Medicine in Houston; Lindsey R. Baden, M.D., principal investigator of the NIAID-funded Harvard HIV Vaccine Clinical Trials Unit at Brigham and Women’s Hospital in Boston; and Brandon Essink, M.D., principal investigator and medical director of Meridian Clinical Research.
More detailed information about the trial, including more comprehensive data, will be available in a forthcoming report. For more information about the trial, visit clinicaltrials.gov and search identifier NCT04470427.
RNA vaccines
- Unlike a normal vaccine, RNA vaccines work by introducing an mRNA sequence (the molecule which tells cells what to build) which is coded for a disease specific antigen, once produced within the body, the antigen is recognised by the immune system, preparing it to fight the real thing
- RNA vaccines are faster and cheaper to produce than traditional vaccines, and a RNA based vaccine is also safer for the patient, as they are not produced using infectious elements
- Production of RNA vaccines is laboratory based, and the process could be standardised and scaled, allowing quick responses to large outbreaks and epidemics
- Most current research is into RNA vaccines for infectious diseases and cancer, for which there are several early-stage clinical trials, there is also some early research into the potential of RNA vaccines for allergies
- There is still a lot of work to be done before mRNA vaccines can become standard treatments, in the meantime, we need a better understanding of their potential side effects, and more evidence of their long term efficacy
What are RNA vaccines and how do they work?
Conventional vaccines usually contain inactivated disease-causing organisms or proteins made by the pathogen (antigens), which work by mimicking the infectious agent. They stimulate the body’s immune response, so it is primed to respond more rapidly and effectively if exposed to the infectious agent in the future.
RNA vaccines use a different approach that takes advantage of the process that cells use to make proteins: cells use DNA as the template to make messenger RNA (mRNA) molecules, which are then translated to build proteins. An RNA vaccine consists of an mRNA strand that codes for a disease-specific antigen. Once the mRNA strand in the vaccine is inside the body’s cells, the cells use the genetic information to produce the antigen. This antigen is then displayed on the cell surface, where it is recognised by the immune system.
How are RNA vaccines produced and administered?
A major advantage of RNA vaccines is that RNA can be produced in the laboratory from a DNA template using readily available materials, less expensively and faster than conventional vaccine production, which can require the use of chicken eggs or other mammalian cells.
RNA vaccines can be delivered using a number of methods: via needle-syringe injections or needle-free into the skin; via injection into the blood, muscle, lymph node or directly into organs; or via a nasal spray. The optimal route for vaccine delivery is not yet known. The exact manufacturing and delivery process of RNA vaccines can vary depending on the type.
Types of RNA vaccine
- Non-replicating mRNAThe simplest type of RNA vaccine, an mRNA strand is packaged and delivered to the body, where it is taken up by the body’s cells to make the antigen.
- In vivo self-replicating mRNAThe pathogen-mRNA strand is packaged with additional RNA strands that ensure it will be copied once the vaccine is inside a cell. This means that greater quantities of the antigen are made from a smaller amount of vaccine, helping to ensure a more robust immune response.
- In vitro dendritic cell non-replicating mRNA vaccineDendritic cells are immune cells that can present antigens on their cell surface to other types of immune cells to help stimulate an immune response. These cells are extracted from the patient’s blood, transfected with the RNA vaccine, then given back to the patient to stimulate an immune reaction.
Benefits
Benefits of mRNA vaccines over conventional approaches are1:
- Safety: RNA vaccines are not made with pathogen particles or inactivated pathogen, so are non-infectious. RNA does not integrate itself into the host genome and the RNA strand in the vaccine is degraded once the protein is made.
- Efficacy: early clinical trial results indicate that these vaccines generate a reliable immune response and are well-tolerated by healthy individuals, with few side effects.
- Production: vaccines can be produced more rapidly in the laboratory in a process that can be standardised, which improves responsiveness to emerging outbreaks.
Important challenges
The methods to make mRNA vaccines can be very effective. However, there are technical challenges to overcome to ensure these vaccines work appropriately:
- Unintended effects: the mRNA strand in the vaccine may elicit an unintended immune reaction. To minimise this the mRNA vaccine sequences are designed to mimic those produced by mammalian cells.
- Delivery: delivering the vaccine effectively to cells is challenging since free RNA in the body is quickly broken down. To help achieve delivery, the RNA strand is incorporated into a larger molecule to help stabilise it and/or packaged into particles or liposomes.
- Storage: many RNA vaccines, like conventional vaccines, need to be frozen or refrigerated. Work is ongoing to reliably produce vaccines that can be stored outside the cold chain, since these will be much more suitable for use in countries with limited or no refrigeration facilities.
How could RNA vaccines be used for human health?
The most active areas of research into RNA vaccines are infectious diseases and cancer where there is research ongoing as well as early-stage clinical trials. Work into the use of RNA vaccines to treat allergy is still at the early research stage2.
Infectious diseases
Researchers using conventional approaches have struggled to develop effective vaccines against a number of pathogens, particularly viruses, that cause both acute (Influenza, Ebola, Zika) and chronic (HIV-1, herpes simplex virus) infection. RNA vaccines are being explored as a way to more rapidly and cheaply produce vaccines for these diseases, particularly in response to emerging outbreaks. Clinical trials have been carried out or are ongoing on mRNA vaccines for influenza, cytomegalovirus, HIV-1, rabies and Zika virus.
Case study: A recent study3 explored the use of programmable self-replicating RNA vaccines, delivered in a nanoparticle, for a range of infectious diseases including Ebola virus, H1N1 Influenza and Toxoplasma gondii, which were effective in mice. These vaccines can be manufactured in approximately one week and made against a range of diseases, demonstrating potential terms of swift response to disease outbreaks.
Cancer vaccines
Cancer vaccines are a form of immunotherapy, where the vaccine triggers the immune system into targeting the cancer. Both dendritic cell vaccines and personalised cancer vaccines, where the RNA sequence in the vaccine is designed to code for cancer-specific antigens, are being explored. Over 50 clinical trials are listed on clinicaltrials.gov for RNA vaccines in a number of cancers, including blood cancers, melanoma, glioblastoma (brain cancer) and prostate cancer.
Case study: Researchers sequenced the genomes of tumours from patients with melanoma. They made RNAs coding for mutant proteins, specific to the patients’ cancers, that could generate an immune response and made these into patient-specific vaccines. Eight out of thirteen people vaccinated stayed tumour free up to two years later4
RNA vaccines – who’s involved?
There are a number of companies and initiatives with an interest in RNA vaccines including the Merit Consortium, which is a European initiative to develop cancer vaccines, while UniVax is a research collaboration to develop a universal influenza vaccine. Companies such as Moderna Therapeutics, CureVac and BioNTech, are involved in phase I trials of RNA vaccines in cancer and infectious disease
. These companies are also exploring the broader use of RNA therapeutics for diseases where important proteins are missing or defective and mRNA treatments could be used to express a functional copy of the protein.
Harnessing RNA vaccines for health – what are the challenges and key considerations?
- Research and clinical trials: further research is needed to address technical hurdles such as vaccine stability and delivery. It is not yet certain which production method(s) are currently the best. Clinical trial data is limited – more long-term studies are needed to determine the effectiveness of RNA vaccines.
- Production: vaccine production is currently small scale and it is not clear if current methods are capable of epidemic-level vaccine production.
- Resources: the personalised approach for cancer vaccines is time and resource intensive and work is needed to determine if this approach is cost-effective.
- Safety: better understanding of vaccine adverse effects is needed – these can include inflammation or autoimmune reactions.
- Pardi N, Hogan MJ, Porter FW, et al. mRNA vaccines – a new era in vaccinology. Nat Rev Drug Discov. 2018; 17(4): 261-279.
- Weiss R, Scheiblhofer S, Thalhamer, J. Generation and Evaluation of Prophylactic mRNA Vaccines Against Allergy. Methods Mol Biol. 2017; 1499: 123-139.
- Chahal JS, Kahn OF, Cooper CL, et al. Dendrimer-RNA nanoparticles generate protective immunity against lethal Ebola, H1N1 influenza, and Toxoplasma gondii challenges with a single dose. Proc Natl Acad Sci USA. 2016; 113(29): E4133-42.
- Sahin U, Derhovanessian E, Miller M, et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature. 2017; 547(7662): 222-226.
Vaccine Development Strategies
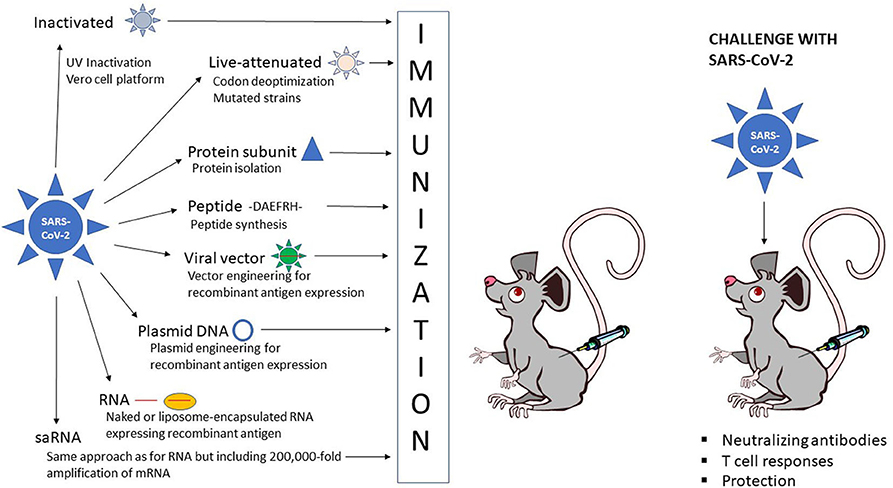
The different strategies for vaccine development against COVID-19 can be divided into three categories: inactivated and live-attenuated viruses, protein subunit and peptide vaccines, and recombinant vaccines based on viral, DNA and RNA delivery (Figure 1).
Obviously, each approach exists with its own variations and engineered modifications as described in more detail below.
 , live-attenuated SARS-CoV-2
, live-attenuated SARS-CoV-2  , protein subunit
, protein subunit  , peptide, -DAEFRH- viral vector expressing SARS-CoV-2 antigen
, peptide, -DAEFRH- viral vector expressing SARS-CoV-2 antigen  , DNA plasmid expressing SARS-CoV-2 antigen
, DNA plasmid expressing SARS-CoV-2 antigen  , naked RNA
, naked RNA  or liposome-encapsulated RNA expressing SARS-CoV-2 antigen
or liposome-encapsulated RNA expressing SARS-CoV-2 antigen  .
.Inactivated and Live-Attenuated Vaccines
In the context of inactivated viruses, it is important that infectious viruses applied for vaccine development are completely inactivated for safety reasons, while the viral epitopes targeted for protective immunity should be conserved to enable high quality antigen production (Delrue et al., 2012).
The virus inactivation process can be hampered by virus aggregate formation, protein crosslinking, denaturation and degradation, which should be addressed before vaccine administration. One approach has been to prepare UV-inactivated virus on a large scale (Tsunetsugu-Yokota, 2008).
For instance, UV-inactivated SARS-CoV was prepared under Biosafety Level 3 (BSL3) regulation including virus expansion, titration, inactivation, and ultracentrifugation, which is also applicable to newly emerging viruses. A versatile Vero cell platform has been established for a wide range of vaccines, including polio virus (Barrett et al., 2017).
Optimization of the platform to include a double inactivation procedure has ensured the highly robust inactivation of novel emerging viruses such as influenza virus, West Nile virus, Chikungunya virus (CHIKV), Ross River virus, SARS-CoV and Zika virus.
Related to live-attenuated viruses, they represent some of the most successful cost-effective interventions in medical history including eradication of smallpox in 1980 (Minor, 2015). Live-attenuated vaccines have functioned well for acute disease, whereas chronic infections such as HIV have been more challenging due to safety and efficacy issues.
The capability of live-attenuated vaccines to elicit humoral and cell-mediated immune responses rely on their physicochemical stability (Tlaxca et al., 2015). Important factors include formulation design, types of robust dosage forms, routes of delivery and distinction between inactivated and live-attenuated vaccines.
An interesting approach evaluated for the prototypic arenavirus lymphocytic choriomeningitis virus (LCMV) comprises codon deoptimization of the surface glycoprotein (GP), which demonstrated wildtype like propagation in cultured cells despite barely detectable expression of GP (Cheng et al., 2017). The codon deoptimized LCMV was highly attenuated in vivo but induced complete protection against lethal challenges with wildtype LCMV, showing a good safety profile and efficacy for a live-attenuated vaccine.
Protein Subunit and Peptide Vaccines
Protein subunit vaccines date back to the time before recombinant protein expression when parainfluenza type 3 (PI-3) virus glycoproteins were isolated by their sedimentation rates after ultracentrifugation and used for immunization of mice and lambs (Morein et al., 1983).
The 30S protein micelles induced high antibody responses as well as provided protection against pneumonia caused by the PI-3 virus. Since then, vaccine development has relied on recombinantly expressed protein subunits for large-scale production in sufficiently pure form for application as safe and effective vaccines (Francis, 2018).
In the context of protein subunit-based vaccines, small protein domains can facilitate and stabilize protein trimerization, which has been demonstrated to enhance their immunogenicity (Morris et al., 1999). Typically, the isoleucine zipper (IZ)3 based on the Saccharomyces cerevisiae GCN4 transcriptional activator (Harbury et al., 1994) and the foldon domain (Fd) of the bacteriophage T4 fibritin protein (Güthe et al., 2004) have been widely used. However, their immunogenicity has been of concern as repeated IZ- or Fd-specific administration could lead to systemic clearance and decreased therapeutic efficacy (Baker et al., 2010).
To address this problem, an IZ variant with four potential N-linked glycosylation sites (PNGS) in the heptad repeat domain were designed, which did not affect protein trimerization but induced significantly lower IZ-specific antibody responses in immunized animals when fused to two HIV-Env and influenza virus hemagglutinin (HA) antigens (Sliepen et al., 2015).
Moreover, the immune response against HIV-Env and influenza virus HA were not affected. This strategy referred to as molecular clamp technology has been applied for preclinical studies on COVID-19 vaccines as described below.
In the case of peptide vaccines, it was demonstrated in the 1980s for foot-and-mouth disease virus (FMDV) that peptides from two regions of the viral protein 1 (VP1) can induce high levels of neutralizing antibodies in guinea pigs, rabbits and cattle (Bittle et al., 1982). Furthermore, a single injection protected guinea pigs from challenges with lethal doses of FMDV. The relatively small molecular size of peptides renders them poor immunogens and it requires coupling to carriers to enhance the immunogenicity (Francis, 2018).
For example, FMDV peptides fused to the N-terminus of β-galactosidase have been engineered, which was known to contain several helper T cell sites for increased immune responses (Francis et al., 1987). Furthermore, it was demonstrated that vaccine candidates with a single copy of the VP1 peptide elicited only low levels of neutralizing antibodies, whereas 2–4 copies provided protection of immunized animals against challenges with FMDV (Broekhuijsen et al., 1986).
In the case of proteins containing two copies, 2 mg of peptide was sufficient for achieving protection, while only 0.8 mg of the four-copy peptide was needed. Another approach involves the production of structures similar to virus-like particles (VLPs) with repeated epitopes on the surface (Clarke et al., 1987). In this context, it was demonstrated that immunogenic FMDV VP1 epitopes linked to hepatitis B virus core antigen (HBcAg) fusion particles were 100-fold more immunogenic than free disulfide dimer synthetic peptides containing B- and T-cell sites and 10 times more immunogenic than carrier-linked peptides.
Viral Vector-Based Vaccines
Viral vectors have been commonly used as delivery vehicles for vaccines (Lundstrom, 2017). The spectrum of vectors used in vaccine development is wide including adenoviruses (Ad), lentiviruses, poxviruses, parainfluenza viruses and particularly self-amplifying RNA (saRNA) viruses such as alphaviruses, flaviviruses, rhabdoviruses, and measles viruses.
The unique feature of saRNA viruses relates to the expression of the non-structural replicase genes, formation of the replicase complex and extreme RNA replication, i.e., self-amplification in the cytoplasm (Lundstrom, 2019). Depending on the polarity of the ssRNA genome of saRNA viruses, the positive strand viral RNA (alphaviruses, flaviviruses) can be directly translated in the cytoplasm or the minus strand (rhabdoviruses, measles viruses) has to be copied to a positive strand first.
It is estimated that the RNA is amplified approximately 200,000 after entering the host cell cytoplasm, making saRNA virus vectors attractive for vaccine development. Another advantage of saRNA viruses relates to the flexibility of utilization of recombinant particles, RNA replicons or DNA plasmid-based vectors.
Independent of which viral vector delivery system is used, the target antigen is introduced into an appropriate expression vector, which then can be subjected to expression verification studies in cell lines and administered for in vivo evaluation in animal models.
In any application of viral vectors, it is important to pay special attention to safety aspects and therefore addressing issues related to target of expression, potential spread of virus, duration of expression, chromosomal integration, vector immunogenicity, and adverse events related to viral delivery vector or therapeutic product.
In the case of target of expression, the route of administration plays an important role as has been seen by evaluation of intramuscular, intradermal, intravenous, intranasal and oral administration using classic needle-based, needle-free and electroporation-based technologies (Zheng et al., 2018; Criscuolo et al., 2019). The spread of virus, duration of expression and chromosomal integration are strongly influenced by the type of viral vector used.
Typically, vectors such as Ad and alphaviruses known to generate transient expression have been favored for immunization studies and although replication-deficient vectors have demonstrated efficacy, introduction of replication-proficient vectors has provided extended but controlled spread of antigen expression. As many viruses possess immunogenic structural proteins, efforts have been made to develop second and third generation vectors, where non-essential viral sequences have been deleted (Fukuhara et al., 2016).
DNA-Based Vaccines
Since the development of efficient recombinant technologies, DNA-based vaccine approaches have become a reality due to the easy handling of DNA plasmids and straightforward manufacturing and stability of highly purified DNA preparations (Lee et al., 2018).
The delivery of DNA vaccines can be by intramuscular injection in the form of naked plasmid DNA (Wolff et al., 1990). Alternatively, electroporation (Hooper et al., 2014), gene gun (McBurney et al., 2016), and liposome (Lundstrom and Boulikas, 2003) or polymer-based (polysaccharides and chitosan) (Sunshine et al., 2011) nanoparticles can be used.
In addition, polysaccharide-based adjuvants and also chitosan can enhance the immunogenicity of vaccines (Barhate et al., 2014). Importantly, to function, DNA plasmid vectors need to be transported to the cell nucleus, which can be facilitated by engineering of nuclear localization signals into the vector (Xu et al., 2016).
In the context of gene expression from DNA vectors, the use of minicircle DNA has been demonstrated to increase therapeutic biosafety as bacterial sequences are removed from the parental plasmid leaving only the gene of interest and the promoter/terminator sequences in the construct (Darquet et al., 1997).
Additionally, it has been shown that minicircles can improve the immunogenicity of DNA vaccines by inducing 10–1,000-fold increase in long-term transgene expression both in vitro and in vivo in comparison to conventional plasmid DNA (Huang et al., 2009). Moreover, studies on combinations of promoters/enhancers and post-translational regulatory elements have been conducted for optimized transgene expression (Sun et al., 2009; Shen et al., 2015).
Another approach comprises codon optimization, where low-frequency eukaryotic codons in the foreign DNA are identified and replaced for high-frequency codons (Grantham et al., 1980; Nagata et al., 1999). It has been demonstrated that codon-optimized DNA vaccines can enhance immunogenicity in mice and chickens (Stachyra et al., 2016). Various synthetic biology methods have also been developed to control gene expression profiles through engineered inducers within genetic circuits, which could potentially enable the regulation of the intensity and type of immune responses (Deans et al., 2012).
Although more than 500 clinical trials have been conducted or are in progress using DNA vaccines, no DNA-based human vaccine has been approved yet (Lee et al., 2018). However. a DNA vaccine against influenza virus H5N1 in poultry has received conditional approval by the USDA (Jazayeri and Poh, 2019).
In the context of human DNA vaccines, clinical trials have demonstrated that neither chromosomal integration of plasmid DNA nor development of anti-DNA antibodies occur. In attempts to improve immune responses, transfection efficiency needs to be improved using higher DNA doses (Liu and Ulmer, 2005). Moreover, prime-boost regimen with a DNA vaccine and a recombinant modified vaccinia virus Ankara (MVA) has proven useful for eliciting antibodies and T cell responses for a HIV vaccine candidate (Thompson et al., 2016).
In another approach, enhanced immune responses were achieved for DNA vaccines by application of intradermal electroporation (Nilsson et al., 2015). Overall, DNA vaccines provide a potentially promising alternative for COVID-19 vaccine development as presented below for preclinical studies and clinical trials.
RNA-Based Vaccines
In addition to DNA-based vaccines, application of RNA in the forms of mRNA and saRNA vectors has recently received increased attention (Lundstrom, 2018). In the case of mRNA-based vaccines, the immediate translation of antigens in the cytoplasm of target cells provides the means for rapid immune responses. However, mRNAs are highly sensitive to degradation due to their single-stranded structure and the presence of RNases, which has resulted in different approaches for improving RNA stability (Brawerman, 1974; Burgess, 2012).
These include the incorporation of anti-reverse cap analogs (ARCAs) in the RNA, which doubled the transcription efficiency (Stepinski et al., 2001) and improved the levels and duration of protein expression in cells transfected with ARCA-capped in vitro transcribed RNA (Zohra et al., 2007). RNA stabilization can also be obtained by engineering the poly(A) tail at the 3′ end of mRNAs based on the synergistic interaction between poly(A) and the 5′ m7G cap sequences by binding to the poly(A) binding protein (PABP) (Bernstein et al., 1989).
Poly(A) tail engineering has demonstrated that increase in length enhanced polysome formation also showing an impact on protein expression levels (Munroe and Jacobson, 1990). The optimal length of the poly(A) tail has been suggested to be between 120 and 150 nucleotides (Holtkamp et al., 2006; Mockey et al., 2006). Furthermore, 5′ and 3′ end untranslated regions (UTRs) play an important role in mRNA stability and transport from the nucleus (van der Velden and Thomas, 1999; Bashirullah et al., 2001).
Chemical modification by introduction of modified pseudouridine has also resulted in improved RNA stability and enhanced translation (Kariko et al., 2005, 2008). Another approach comprises high liquid chromatography purification of in vitro transcribed RNA for removal of double-stranded RNA contaminants in attempts to reduce the production of type 1 interferon and pro-inflammatory cytokines (Kariko et al., 2011).
As with any other approach, delivery is a major issue of concern for RNA-based vaccines, not the least because of the stability issues related to RNA. Although naked RNA is far from optimal for delivery, intramuscular mRNA injections have demonstrated successful in vivo reporter gene (Wolff et al., 1990) and carcinoembryonic antigen (CEA) expression eliciting anti-CEA antibody responses in mice (Conry et al., 1995).
However, the exposure of RNA to rapid degradation by ubiquitous RNases remains a problem (Probst et al., 2006; Houseley and Tollervey, 2009). Naked mRNA can also act as an adjuvant (McNamara et al., 2015), where antigen-encoding RNA elicits antigen-specific T and B cell immune responses (Pardi and Weissman, 2017). Moreover, co-stimulatory molecules like CD40L when co-expressed with mRNA can further enhance the immunogenicity (Schlake et al., 2012).
To improve and facilitate mRNA delivery and penetration of cell membranes, gene gun-based systems including mRNA coated in gold particles have been applied (Dileo et al., 2003). In the context of melanoma, mRNA expressing the melanocyte self-antigen TRP2 fused to EGFP was delivered by gene gun, which led to antigen-specific humoral and cellular immune responses and protection against B16 melanoma lung metastasis in a mouse model (Steitz et al., 2006).
Protamine condensation of mRNA has also been demonstrated to provide protection against RNA degradation (Sköld et al., 2015) and can further stimulate antigen-specific IgG antibodies and activate specific cytotoxic T lymphocyte (CTL) responses (Hoerr et al., 2000). Obviously, encapsulation has provided improved means for stability and delivery of RNA by application of liposomes and biopolymers.
For instance, the cationic liposome DOTAP can provide protection against nuclease degradation and enhance cellular uptake (Phua et al., 2013). Intradermal administration of DOTAP liposomes into mouse ear pinna, protected animals against subcutaneous tumor challenges with EG7-OVA cells (Hess et al., 2006). Moreover, DOTAP/DOPE formulations showed fusogenic properties, which resulted in enhanced CTL responses.
The important role of the professional antigen presenting dendritic cells (DCs) in stimulation of immune responses has also accelerated the formulation of nanoparticles optimized for targeting DCs (Ahmad et al., 2017). Immunization with DCs transfected with mRNA expressing CEA showed good tolerance in pancreatic cancer patients in a phase I study resulting in a complete response in one patient, minor responses in two individuals and stable disease in three patients with progressive disease in the remaining 18 patients (Morse et al., 2003). Moreover, DCs transfected with mannosylated, histidylated lipoplex nanoparticles expressing tumor antigen mRNA showed enhanced inhibition of B16F10 melanoma growth and prolonged survival in mice (Perche et al., 2011).
Finally, in the context of RNA-based vaccines, application of saRNAs has opened new possibilities. The cytoplasmic RNA amplification generates superior quantities of mRNA providing improved immune responses with the requirement of significantly lower doses of RNA (Lundstrom, 2019).
Although naked saRNA has been demonstrated to provide good immune responses, formulations with different lipids such as ionizable C12-200 and cationic DDA and DOTAP generated lipid nanoparticles (LNPs) with exterior or interior saRNAs (Blakney et al., 2019). The LNPs formulated with cationic lipids protected saRNA from degradation even when the saRNA was absorbed to the surface. Both saRNA LNPs encapsulated with cationic and ionizable lipids showed transfer in vitro and in vivo and induced equivalent antibody responses against HIV-1 Env gp140.
Journal information: New England Journal of Medicine



{kind=link}
[…] The Moderna COVID-19 vaccine causes strong antibody response remains 90 days… […]
[…] The Moderna COVID-19 vaccine causes strong antibody response remains 90 days… […]