










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



An international research team led by the University of British Columbia (UBC) has uncovered for the first time the importance of a small gland tucked behind the sternum that works to prevent miscarriage and diabetes in pregnant women.
The organ in question is the thymus, identified in a study published today in the journal Nature as playing a significant role in both metabolic control and immunity in pregnancy.
How the immune system adapts to support mother and fetus has puzzled researchers for decades. The study – conducted by an international research team, including UBC’s Dr. Josef Penninger – reveals an answer.
The researchers have found that female sex hormones instruct important changes in the thymus, a central organ of the immune system, to produce specialized cells called Tregs to deal with physiological changes that arise in pregnancy.
The researchers also identified RANK, a receptor expressed in a part of the thymus called the epithelium, as the key molecule behind this mechanism.
“We knew RANK was expressed in the thymus, but its role in pregnancy was unknown,” says the study’s senior author Dr. Penninger, professor in the department of medical genetics and director of the Life Sciences Institute at UBC.
To get a better understanding, the authors studied mice where RANK had been deleted from the thymus.
“The absence of RANK prevented the production of Tregs in the thymus during pregnancy. That resulted in less Tregs in the placentas, leading to elevated rates of miscarriage,” says the study’s lead author Dr. Magdalena Paolino, assistant professor in the department of medicine at the Karolinska Institutet.
The findings also offer new molecular insights into the development of diabetes during pregnancy, known as gestational diabetes, a disease that affects approximately 15 percent of women in pregnancy worldwide, and about which scientists still know little.
In healthy pregnancies, the researchers found that Tregs migrated to the mother’s fat tissue to prevent inflammation and help control glucose levels in the body.
Pregnant mice lacking RANK had high levels of glucose and insulin in their blood and many other indicators of gestational diabetes, including larger-than-average young.
“Similar to babies of women with diabetes in pregnancy, the newborn pups were much heavier than average,” says Dr. Paolino.
The deficiency of Tregs during pregnancy also resulted in long-lasting, transgenerational effects on the offspring. The pups remained prone to diabetes and overweight throughout their life spans.
Giving the RANK-deficient mice thymus-derived Tregs isolated from normal pregnancies reversed all their health issues, including miscarriage and maternal glucose levels, and also normalized the body weights of the pups.
The researchers also analyzed women with diabetes in pregnancy, revealing a reduced number of Tregs in their placentas, similar to the study on mice.
“The discovery of this new mechanism underlying gestational diabetes potentially offers new therapeutic targets for mother and fetus in the future,” says co-author Dr. Alexandra Kautzky-Willer, a clinician-researcher based at the Medical University of Vienna.
“The thymus changes massively during pregnancy and how such rewiring of an entire tissue contributes to a healthy pregnancy has been one of the remaining mysteries of immunology,” adds Dr. Penninger.
“Our work over many years has now not only solved this puzzle – pregnancy hormones rewire the thymus via RANK – but uncovered a new paradigm for its function: the thymus not only changes the immune system of the mother so it does not reject the fetus, but the thymus also controls metabolic health of the mother.
“This research changes our view of the thymus as an active and dynamic organ required to safeguard pregnancies,” says Dr. Penninger.
Structure and Function
The thymus is a superior mediastinal retrosternal organ. It is bilobed and has two subcomponents: the cortex and the medulla and is made up of epithelial, dendritic, mesenchymal and endothelial cells.[3] The thymus is one organ which has already reached its maturity in utero and involutes as people age. Involution of thymus involves changes in its architecture, as it loses its organized structure replaced by adipose tissue as it becomes functionally less active.
Several studies since the 1960s demonstrate that the thymus is necessary for life. Mice that received a thymectomy had an immunodeficiency with a decreased number of lymphocytes.[1]
The thymus is the organ primarily responsible for the production and maturation of immune cells; including small lymphocytes that protect the body against foreign antigens. The thymus is the source of cells that will live in the lymphoid tissues and supports their maturation and proper function.
Positive selection is used by the thymus to select self-antigen recognizing t-cells to be destined for apoptosis. The thymus is where T-cells get exposure to self-antigen, and 95% of all created T cells undergo apoptosis due to their recognition of self-antigen. The non-reactive T-cells then go through negative selection for those that bind to antigen with high affinity.[1]
Only lymphocytes that pass both positive and negative selection are allowed to travel out of the thymus. These T-cells are activated by bacteria, viruses or other foreign antigens and then undergoes mitosis. After the pathogen dies, the cells go through apoptosis and the ones that do not continue as memory cells.
These cells allow the immune system to respond quicker and stronger the next time they interact with the same antigen.[1] Hassall’s bodies, cells unique to the thymus, are involved in maturing thymocytes and clearing apoptotic cells. They are a vital part of lymphopoiesis.[2]
Embryology
Originally derived from the ventral third pharyngeal pouch,[2] the thymus grows from embryogenesis to 3 years of age and then involutes during puberty.[1] During embryogenesis, the thymus migrates from the third pharyngeal pouch down into the superior mediastinum posterior to the manubrium. The thymus is large in infants and young children and coalesces over time, and thymic tissue is replaced by fat by early adulthood.[2] Thymic involution is suggested to be caused by the increased levels of androgens present in the bloodstream during puberty.[2]
Blood Supply and Lymphatics
The thymus’ blood supply is complicated and widely varies. Most often the blood is supplied by the inferior thyroid, internal thoracic, pericardiacophrenic or anterior intercostal arteries. Rarely, the thymus can obtain blood from the middle thyroid artery.[2] Laterally, the thymus receives blood from branches of the internal mammary artery.
These branches are named the lateral thymic arteries; they vary in number and are asymmetric. Posterior thymic arteries derive from the brachiocephalic artery and the aorta; however, they are rare. Accessory thymic arteries are diverse but have been documented to originate from the thyrocervical trunk, subclavian or superior thyroid arteries.
Venous drainage variation is common, but most often the thymus is drained by left brachiocephalic and internal thoracic tributary veins.[2] Thymic venous supply runs in the interlobular septa, into the thymic capsule, and leaves the cortex via a plexus on the posterior side of the organ. These veins then join together and drain each lobe separately.[2]
Nerves
Sympathetic innervation of the thymus originates from the superior cervical and stellate ganglion. These fibers travel in a plexus along large blood vessels until they enter the thymic capsule. Parasympathetic fibers arise from the vagus, recurrent laryngeal and phrenic nerves. Several rodent studies have found that thymocytes respond to stimuli via norepinephrine, dopamine, acetylcholine, neuropeptide Y, vasoactive intestinal peptide, calcitonin gene-related peptide, and substance P.[2]
Muscles
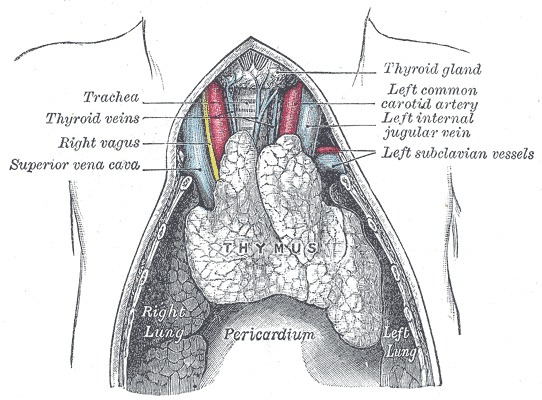
The thymus sits in the mediastinum just posterior to the manubrium. The muscles that depress the hyoid bone that attach to the sternum are near the thymus. These muscles include the sternohyoid and sternothyroid, and both muscles are bilateral. The thyrohyoid and sternocleidomastoid muscles are close to any ectopic thymic tissue or any superior extensions of the thymus. The thymus also lies anterior to the cardiac muscle and pericardium.[4]
Physiologic Variants
Variants in the number of lobes, size, and location of the thymus are common. The most common anatomic variant is an extension reaching up to the thyroid gland.[2] During descent of the thymus tissue may implant along the way and is then defined as an ectopic thymus. Fifty percent of people have ectopic thymic tissue. This variant is typically located in the anterior cervical region, deep to the sternocleidomastoid muscle, anterior to the carotid sheath, and can expand into the retropharyngeal space.[2] Half of these masses connect to the thymus in the mediastinum.[2]
Surgical Considerations
The thymus poses difficulty for surgeons due to its high variation in size and arterial supply. Imaging of the gland is also difficult and rarely provides surgeons any insight. On standard chest radiographs, the thymus is rarely discernible as it gets lost in the cardiac silhouette. The gland has smooth borders and is more visible in x-rays of infants and young children. Ultrasound is mostly used to assess the thymic parenchyma, and CT scan is most helpful to assess the location, size, shape, and its relationship to other structures.[2]
An ectopic thymus can be confused for lymphadenopathy or a tumor. Since the difference is difficult to discern clinically, their benign nature is most often confirmed after resection. Another complication of ectopic thymic tissue is that it can compress nearby structures; this can cause swelling, decreased blood flow, discomfort, and impaired thyroid function. Resection of these masses possesses surgical difficulty due to many adhering to the carotid sheath and in close proximity to vital pharyngeal muscles and phrenic nerve.[1]
Clinical Significance
Insulin is known to play an essential role in thymic growth. Insulin, growth hormone and insulin-like growth factor increase the development of lymphocytes and insulin can be found in the medulla of the thymus. Type 1 diabetes adversely affects the thymus; these patients will have a decreased immune system in addition to their diabetes and other related complications. The supplementation with insulin can be protective of their thymic function and preserve their immune system maturation.[2]
Thymus hyperactivity secondary to hyperplasia of the organ is common in myasthenia gravis. However, thymus tumors, lymphomas, systemic lupus, or hyperthyroidism can also cause this clinical finding. Patients with thymus hyperactivity will have pallor, lymphadenopathy, rhinorrhea, and tonsillitis. This condition’s treatment includes vitamins A and D, calcium, and iodine. Thalassotherapy, thymus radiotherapy, and heliotherapy may also be treatments.[1]
Myasthenia gravis (MG) is an autoimmune pathology resulting in muscle weakness. The thymus produces antibodies that interrupt the signaling of acetylcholine at the motor end plate. Patient’s muscle strength with worsened with continued contractions and this is a clinical finding that differentiates MG from Lambert-Eaton syndrome.
Thymic hypertrophy in MG is so common that it is considered a diagnostic criterion; along with the antibodies found in the blood to the acetylcholine receptors and anti-muscarinic antibodies. Physicians may use an MRI or CT scan to evaluate the size of the thymus.[1] MG is treated depending on the severity of the disease.
Treatments range from immunosuppression and corticosteroids to surgical thymectomy. In some patients, only pyridostigmine bromide, a medication that slows the breakdown of acetylcholine, is necessary for symptom control. In patients with this condition, it is essential to keep in mind the potential drug exacerbations of disease when treating acute illness or comorbidities.[1]
In contrast, atrophy of the thymus is present in several congenital conditions. DiGeorge syndrome is when the thymus fails to form in utero. This agenesis results in an immature immune system and recurrent infections. Severe combined immunodeficiency (SCID) is a genetic disorder where the thymus disappears early in childhood, and the patient lacks T and B cells. These children are also at significant risk for severe, recurrent infections.[1]
Other Issues
As humans age, and their thymus regresses, they have an increased susceptibility for disease. This decrease in thymus size and function leads to decreased circulating T cells and alteration of their role. This change in function can increase autoimmune diseases, bacterial and viral infections, and neoplasms. Restoring thymic function or intervening before involution could maintain the immune system throughout adult life.[2] The thymus is a current area of research with great promise.
One study from Scottish researchers found they were able to re-grow an adult mouse thymus from stem cells. This new organ began to produce T-cells.[1] Duke University in Durham, North Carolina, has successfully performed thymus transplants on children with DiGeorge syndrome.[1] Thymus research poses incredible medical breakthroughs for many diseases and the possibility to revamp adult immune systems.
References
- 1.Zdrojewicz Z, Pachura E, Pachura P. The Thymus: A Forgotten, But Very Important Organ. Adv Clin Exp Med. 2016 Mar-Apr;25(2):369-75. [PubMed]
- 2.Rezzani R, Nardo L, Favero G, Peroni M, Rodella LF. Thymus and aging: morphological, radiological, and functional overview. Age (Dordr). 2014 Feb;36(1):313-51. [PMC free article] [PubMed]
- 3.Yan F, Mo X, Liu J, Ye S, Zeng X, Chen D. Thymic function in the regulation of T cells, and molecular mechanisms underlying the modulation of cytokines and stress signaling (Review). Mol Med Rep. 2017 Nov;16(5):7175-7184. [PMC free article] [PubMed]
- 4.Kohan EJ, Wirth GA. Anatomy of the neck. Clin Plast Surg. 2014 Jan;41(1):1-6. [PubMed]
More information: RANK links thymic regulatory T cells to fetal loss and gestational diabetes in pregnancy, Nature (2020). DOI: 10.1038/s41586-020-03071-0 , www.nature.com/articles/s41586-020-03071-0



{kind=link}