










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The study, published today in the Journal of the American Heart Association (JAHA) and led by researchers at the Gerald J. and Dorothy R. Friedman School of Nutrition Science and Policy at Tufts University, used a mathematical simulation to estimate the number and proportion of national COVID-19 hospitalizations that could have been prevented if Americans did not suffer from four major cardiometabolic conditions.
“While newly authorized COVID-19 vaccines will eventually reduce infections, we have a long way to go to get to that point. Our findings call for interventions to determine whether improving cardiometabolic health will reduce hospitalizations, morbidity, and health care strains from COVID-19,” said Dariush Mozaffarian, lead author and dean of the Friedman School.
“We know that changes in diet quality alone, even without weight loss, rapidly improve metabolic health within just six to eight weeks. It’s crucial to test such lifestyle approaches for reducing severe COVID-19 infections, both for this pandemic and future pandemics likely to come.”
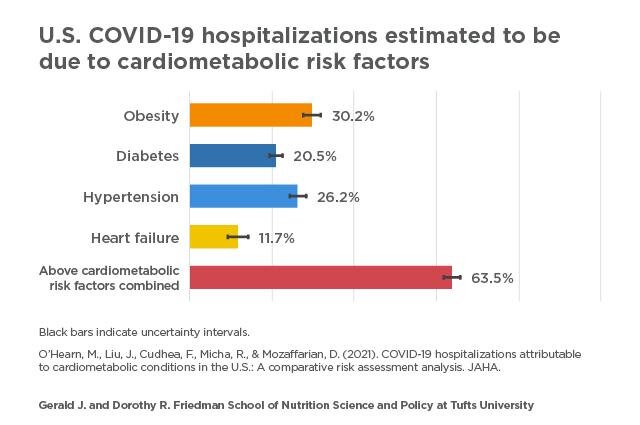
- 30% (274,322) were attributable to obesity;
- 26% (237,738) were attributable to hypertension;
- 21% (185,678) were attributable to diabetes; and
- 12% (106,139) were attributable to heart failure.
In epidemiological terms, the attributable proportion represents the percentage of COVID-19 hospitalizations that could have been prevented in the absence of the four conditions. In other words, the study found the individuals might still have been infected but may not have had a severe enough clinical course to require hospitalization.
When numbers for the four conditions were combined, the model suggests 64% (575,419) of COVID-19 hospitalizations might have been prevented. A 10% reduction in national prevalence of each condition, when combined, could prevent about 11% of all COVID-19 hospitalizations, according to the model.
The four conditions were chosen based on other published research from around the world showing each is an independent predictor of severe outcomes, including hospitalization, among people infected with COVID-19. The specific risk estimates for each condition were from a published multivariable model involving more than 5,000 COVID-19 patients diagnosed in New York City earlier in the pandemic.
The researchers used other national data to model the number of COVID-19 hospitalizations nationally; the distributions of these hospitalizations by age, sex, and race; and the estimated distribution of the underlying comorbidities among adults infected with COVID-19.
They then estimated the proportions and numbers of COVID-19 cases that became severe enough to require hospitalization owing to the presence of one or more of the conditions.
“Medical providers should educate patients who may be at risk for severe COVID-19 and consider promoting preventive lifestyle measures, such as improved dietary quality and physical activity, to improve overall cardiometabolic health. It’s also important for providers to be aware of the health disparities people with these conditions often face,” said first author Meghan O’Hearn, a doctoral candidate at the Friedman School.
The model estimated that age and race/ethnicity resulted in disparities in COVID-19 hospitalizations due to the four conditions. For example, about 8% of COVID-19 hospitalizations among adults under 50 years old were estimated to be due to diabetes, compared to about 29% of COVID-19 hospitalizations among those age 65 and older. In contrast, obesity had an equally detrimental impact on COVID-19 hospitalizations across age groups.
At any age, COVID-19 hospitalizations attributable to all four conditions were higher in Black adults than in white adults and generally higher for diabetes and obesity in Hispanic adults than in white adults.
For example, among adults age 65 and older, diabetes was estimated to cause about 25% of COVID-19 hospitalizations among white adults, versus about 32% among Black adults, and about 34% among Hispanic adults.
When the four conditions were considered combined, the proportion of attributable hospitalizations was highest in Black adults of all ages, followed by Hispanics. For example, among young adults 18-49 years old, the four conditions jointly were estimated to cause about 39% of COVID-19 hospitalizations among white adults, versus 50% among Black adults.
“National data show that Black and Hispanic Americans are suffering the worst outcomes from COVID-19. Our findings lend support to the need for prioritizing vaccine distribution, good nutrition, and other preventive measures to people with cardiometabolic conditions, particularly among groups most affected by health disparities,” Mozaffarian said.
“Policies aimed at reducing the prevalence of these four cardiometabolic conditions among Black and Hispanic Americans must be part of any state or national policy discussion aimed at reducing health disparities from COVID-19.”
etween July 2020 and January 2021, we conducted a literature search in PubMed, Google Scholar, Science Direct, and Scopus for articles published between January 2020 and January 2021 (with an exception to this time range if the article was only used to contextualize general challenges and epidemiology of chronic disease patients). Combinations of the search terms “chronic disease”, “COVID-19”, “cardiovascular disease”, “coronary artery disease”, “heart failure”, “myocardial infarction”, “hypertension”, “chronic obstructive pulmonary disease”, “asthma”, “diabetes”, “epilepsy”, “insomnia”, “obstructive sleep apnea”, “telemedicine”, “drug shortages”, “diet”, “nutrition”, “physical exercise”, “primary care”, “hospitalization”, “fee-for-service”, “capitation”, “mental health”, and “stress” were used to initially retrieve articles. We screened titles and abstracts using the following criteria.
Inclusion criteria were defined as any English-language peer-reviewed primary articles, review articles, or opinion and commentary articles that focused on, or at least included, non-SARS-CoV-2 infected patients with chronic diseases during the COVID-19 pandemic. Exclusion criteria were defined as any sources that did not fit into these criteria, such as articles that focused only on SARS-CoV-2 infected patients with comorbid chronic diseases. Articles that met inclusion criteria were subsequently evaluated in their entirety for content relevancy to our narrative discussion. All authors agreed on the final reference list.
Healthcare Characteristics and Utilization by Individuals with Chronic Conditions During the COVID-19 Pandemic
Primary Care Characteristics and Utilization by Individuals with Chronic Conditions
Primary care serves as a gateway into the healthcare system and promotes better health outcomes for individuals with chronic conditions through monitoring, management, and follow-up. To mitigate the spread of COVID-19 infection, primary care centres around the world concertedly transitioned into remote consultations with ad hoc in-person medical visits. Commonly, this is presented as a three-step framework:
(1) patients are triaged remotely and reviewed for travel history, contact history, and COVID-19 symptoms; (2) patients with chronic diseases or mild COVID-19 symptoms are advised to quarantine at home while routinely consulting with physicians remotely by video, phone, email, etc.; (3) patients with substantially-worsened chronic diseases or severe COVID-19 symptoms who require urgent care are hospitalized.11–15
In theory, this framework optimizes the distribution of personal protective equipment (PPE) and staff to urgently treat individuals with COVID-19 and protects patients with chronic diseases from potential COVID-19 exposure in hospitals and clinics. However, in practice, the efficacy of such measures is largely dictated by the availability of financial and infrastructural resources. A recent cross-sectional study found that within resource-rich settings and consistent access to a regular primary care physician prior to the pandemic, in-person outpatient visits for chronic conditions fell by 60% to 70%, while there was a 60% to 100% increase in video and telephone consultations.16
This smooth shift into remote care resulted in higher patient satisfaction and consistent no-show rates than before the onset of COVID-19, reflecting these patients continued timely and effective access to primary care during the COVID-19 pandemic.16,17 However, even in resource-rich settings, there is a high degree of variability among different communities;18 specifically, inequalities in chronic diseases and the social determinants of health among minority ethnic groups, people living in areas of higher socioeconomic deprivation, individuals living in poverty, and other marginalised groups.19
Further, resource-constrained and low-income settings may force individuals with chronic conditions to either continue in-person medical visits, risking potential COVID-19 exposure or stay at home and seek medical care only after their conditions have substantially worsened.
This stretches existing health inequities for socioeconomically-disadvantaged patients with chronic diseases and has impeded the management of their diseases; thus, worsening health outcomes.20 For example, among people with diabetes in such settings, 80% were concerned with their ability to ensure timely follow-up with clinicians, and more than 70% reported worsening of glycemic control manifesting as higher fasting blood glucose levels, mainly due to their inability to reach primary care clinicians for modulating insulin dosages.21,22
Interestingly, these reductions in face-to-face primary care visits by patients with chronic conditions have substantial financial consequences for healthcare systems. A large-scale modelling study of US outpatient and primary care centres estimated that a conservative 6% reduction in total visit volume leads to a nearly $70,000 (USD) loss per full-time physician and a net $15 billion (USD) loss across all US primary care centres.23
Further, for over half of these clinicians who rely on independent small practices and likely have less capital to smoothly transition into telemedicine, these financial losses could balloon two-fold, (1) risking the closure of their practices or staff layoffs, and (2) suggesting incompatibility of patient-centered care with fee-for-service (FFS) payment.24,25 Weakened primary care systems are likely to adversely impact the quality of care of individuals with chronic conditions for years beyond the COVID-19 pandemic.23
In Ontario (Canada), a survey of 4800 fee-for-service primary care physicians found that nearly 50% had already laid off staff and may need to close their practices unless they receive additional financial support.26 Early evidence suggests that capitation primary care models, which are not reliant on the volume of services but instead on delivering cost-effective care for a specified patient volume, maybe better-suited to ensure the robustness of primary care during COVID-19.24
Capitation primary care physicians may be incentivized to ensure that patients remain healthy to limit any future visits and subsequent care needed.27–29 It has been previously shown that compared to fee-for-service primary care models, capitation may yield higher rates of patients receiving recommended management and favourable health outcomes,30,31 while also reducing admission rates for individuals with chronic conditions.32
A reduction in hospitalization rates due to primary care improvement is especially critical during the COVID-19 pandemic to free resources for the urgent care of individuals with COVID-19. Despite benefits offered by capitation models, a large concern is that capitation primary care providers may be financially-incentivized to avoid enrolling or undertreat patients with chronic conditions, as these patients are associated with recurrent admissions (both virtual and in-person); hence, capitation rates may need to be adjusted for patients with chronic conditions to reflect the higher expected costs.33
Further, the efficacy of different primary care models for patients with chronic conditions during the COVID-19 pandemic remains poorly understood; thus, more research is urgently needed contrasting the efficacy and access to care of capitation models compared to FFS models for patients with chronic conditions, specifically during the COVID-19 pandemic, as well as potential areas of risks for both models.
Reductions in Chronic Disease-Related ED Visits and Hospitalizations
The COVID-19 pandemic also led to significant reductions in hospitalizations, ED visits, and inpatient visits for non-COVID-19 patients with chronic conditions, notably, during the period of March 2020 to April 2020. Individuals with acute myocardial infarction, stroke, heart failure, and other chronic cardiovascular conditions experienced a significant (~40%) decrease in hospital admissions and ED visits during the COVID-19 pandemic compared to baseline.34–39
Rates of heart failure-related hospitalizations decreased 40–50% during the COVID-19 period compared to before;34,40 however, one study found a three-fold increase in mortality related to heart-failure.41 Overall, these trends are concerning, suggesting that patients with chronic cardiovascular conditions tend to avoid in-person medical visits to hospitals, clinics, and ED possibly due to fear of potential COVID-19 exposure.
In a cross-sectional study of 185,000 North American patients, one-third reported cancelling pre-scheduled appointments, and over 40% reported elevated worry regarding in-person medical visits.42 Hypertension and cardiovascular conditions have often been shown as the two leading comorbidities in COVID-19 related mortality, raising the risk two-fold. Therefore, chronic cardiac patients may be especially prudent about minimizing in-person healthcare visits during the COVID-19 pandemic.43–46
Especially vulnerable are elderly patients with chronic conditions. Elderly individuals are at greater susceptibility to COVID-19 infection, worse prognosis following COVID-19 infection, and are also more likely to have one or more non-communicable diseases; thus, they may face heightened levels of instilled fear of COVID-19 exposure during in-person medical visits.47
Further, elderly patients with chronic diseases have a higher prevalence of moderate to severe dementia48,49 and cognitive impairment, which may limit their ability to effectively manage their chronic conditions. People with dementia also face worse health outcomes following COVID-19 exposure, including a nearly 3-fold elevated risk of mortality.50 Altogether, elderly patients are a subset of the chronic disease population that may face especially amplified fear and difficulty maintaining chronic disease healthcare routines due to the COVID-19 pandemic.
Two alternative theories have been proposed to explain reductions in chronic disease-related ED visits and hospitalizations in addition to possible fear of potential COVID-19 exposure due to in-person medical visits. First, the reduction in hospitalizations may also be attributed to the mitigation of other lifestyle and environmental risk factors during quarantine, such as reduced exposure to traffic, air pollution, other respiratory infections (eg, influenza), as well as reduced energy expenditure.35,51
This is supported by a decline in hospitalizations and ED visits for chronic obstructive pulmonary disease (COPD)/asthma and pneumonia during the COVID-19 pandemic, which shares many of these risk factors.37,52,53 Another possible explanation is that the effective shift into telemedicine, coupled with the absence of prior distractions (eg, work, travel, etc.), has led to increased treatment adherence and improved management of chronic conditions.54,55
Deployment of Telemedicine for Chronic Disease Management
Prior to the COVID-19 outbreak, telemedicine had already been distinguished as an effective strategy to monitor and manage chronic illnesses, for example, for patients with heart failure and COPD.56,57 Suddenly, social distancing, quarantine, and hospital restriction measures have forced individuals with chronic conditions to re-envision their routine treatments remotely with ad hoc in-person medical visits.
This has led to widespread and significant increases in telemedicine utilization.58–60 A rapid review found that telemedicine utilization had increased by nearly 90% in the US during the COVID-19 pandemic.61 Common uses of telemedicine include video or phone consultations, allowing individuals with chronic conditions to self-monitor symptoms and send this information to their clinicians, mobile apps, and platforms.55,62
For chronic heart failure patients, virtual care has enabled effective routine monitoring (eg, heart rhythm, blood pressure, O2 saturation) associated with better compliance with treatment rates (51% vs 35%) and follow-up rates than in-person care during COVID-19.63 Among patients with chronic respiratory conditions such as asthma or COPD, remote care has been effective for self-management education (eg, inhaler device training, breathing techniques, recognizing symptoms, forming or complying with action plans, etc.), leading to improved health outcomes.52,64 For people with epilepsy, virtual services like electronic seizure journals, mobile apps, messaging, and video conferencing have led to high patient satisfaction rates, lower no show rates, and better health outcomes.65
Despite these advantages, telemedicine is associated with many barriers to implementation, including (1) limited ability to perform physical exams or ancillary testing, (2) reduced ability to pick up verbal and nonverbal cues, which could result in more diagnostic errors, and (3) a lack of access to technology and limitations inherent to variations in digital literacy, especially in elderly patients for whom chronic conditions are common.64–66 Digital illiteracy is more common among socioeconomically disadvantaged, racialized, older, and rural-residing individuals, which may contribute to lower telemedicine access by these populations.
Consistent with this, rates of telemedicine visits for chronic disease patients have been found to be reduced among those who have lower-income or older age (>60 years), are racialized (Hispanic, Black, Asian/Pacific Islander), living in rural areas, and non-English speaking.67,68 Moreover, previous research has found that among the one in eight Americans who live in poverty, the proportion who own smartphones, have broadband access to the internet, and have basic digital literacy are 30%, 40%, and 50% lower, respectively, than those not living in poverty.69
These findings highlight a public health need to increase the financial and technological accessibility of telemedicine services, especially in the context of the COVID-19 pandemic. Therefore, unless telemedicine services address the above disparities, pre-existing health inequities will be further exacerbated.70 Ultimately, more needs to be done to provide patients with chronic diseases, especially those from socioeconomically disadvantaged groups, with technological and financial resources, such as broadband internet access and digital devices, as well as support to develop digital skills.67
Shortages of Medication Supply for Individuals with Chronic Diseases
During the COVID-19 pandemic, medications supplies have fluctuated due to the global disruption of supply and transportation chains, manufacturing restrictions due to insufficient raw materials or social distancing measures for workers, stockpiling and panic-buying behaviour in some patients, and higher demands to treat or develop clinical trials for COVID-19 patients, which has caused medicine shortages for patients with chronic conditions.71–73
Notably, hydroxychloroquine, which is used for treating chronic autoimmune diseases like lupus and rheumatoid arthritis, faced tripled demand during COVID-19 as a promising therapeutic medication for treating patients with COVID-19, leading to major shortages.74 At the early outbreak period, medications like dapagliflozin and metformin used to treat diabetes,75 and midazolam and propofol, which are sedatives that have been used to treat a chronic respiratory condition such as COPD,76 faced critical shortages due to demand in treating COVID-19 patients on mechanical ventilation.
Among COPD and asthma patients, concerns surrounding the use of nebulizers and non-invasive ventilation in aerosolizing the COVID-19 virus, thus risking exposure to healthcare workers, have substantially increased demand for metered-dose inhalers and subsequently inhaler shortages.77 Medicine shortages will likely lead to treatment interruption and worsening of chronic conditions symptoms if they continue. However, there is still limited evidence of their direct downstream effects on short- and long-term health outcomes in patients with chronic diseases.
Changes in Lifestyle and Related Risk Factors for Individuals with Chronic Conditions
Barriers to Physical Activity and Exercise for Patients with Chronic Diseases During COVID-19
As aforementioned, social distancing and quarantine measures have mitigated the spread of COVID-19. However, this also has collaterally limited opportunities for individuals with chronic conditions to participate in structured exercised programs (eg, group fitness sessions, team sports) as well as in-person physiotherapy programs specific to their conditions.78–80 Alternative exercise strategies have emerged, such as social media, virtual support groups, and mobile fitness apps, which provide a motivating and social environment, helping individuals with chronic conditions attain their physical activity goals and notably prevent obesity.81,82
Studies found that during the COVID-19 pandemic physical activity and exercise declined by approximately 40% in the general population.83,84 Similarly, cross-sectional studies reported that moderate- and high-intensity daily physical activity were decreased by 30 and 11 minutes, respectively, with 70% of participants, including individuals with chronic conditions, reporting overall less physical activity.78,80
Obese patients with chronic diseases are at aggravated risk for cardiovascular, metabolic, and respiratory complications; thus, leading to worse health outcomes for their pre-existing conditions,79 which may result in an even greater instilled fear of potential COVID-19 exposure during in-person medical visits.85
Altogether, it is essential that individuals with chronic conditions ensure adequate levels of regular physical activity during the COVID-19 pandemic to prevent exacerbations of their conditions and promote better health outcomes.86
Psychosocial and Mental Health Considerations for Individuals with Chronic Conditions During COVID-19
A higher prevalence of comorbid mental disorders such as depression, anxiety, and chronic stress has been previously found in individuals with chronic physical conditions.1–3,87 They consistently report more social isolation, uncertainty about the future, and guilt stemming from the actual or perceived physical and psychosocial limitations of their disease. These three outcomes, which may likely be worsened by the COVID-19 pandemic, can exacerbate the morbidity of their chronic disease, creating a vicious cycle.87,88
For individuals with chronic cardiovascular diseases, greater stress levels have been previously documented as a risk factor for atherosclerosis, development of hypertension, and recurrent coronary heart disease,89–91 particularly with a 40–50% elevated incidence of recurrent coronary heart disease.91 A US cross-sectional study found that, compared to the general population, patients with chronic conditions experience higher stress levels due to being at higher risk for worse health outcomes from COVID-19 infection.92
For instance, among patients with epilepsy, elevated stress levels and mental health issues were highly prevalent93,94 with higher seizure frequency during the COVID-19 outbreak, which is consistent with the amplified worry of being unable to receive timely and effective access to primary care and antiseizure medications.95
Correspondingly, in one study, 73% and 40% of patients with epilepsy reported that obtaining routine anti-epilepsy medications and managing stress levels, respectively, were made “more difficult” by the COVID-19 pandemic through a wide array of factors (greater difficulty with reaching their epilepsy healthcare providers, difficulty with maintaining normal sleep routines, greater difficulty with obtaining anti-epilepsy medications and with routinely taking these medications).87 Notably, one-third of patients in this study reported increased seizure frequency during the COVID-19 pandemic.95
Sleep Disruption and Disorders for Individuals with Chronic Conditions During COVID-19
The COVID-19 pandemic significantly amplified the frequency and severity of sleep disruptions. Notably, occurrences of clinically meaningful sleep difficulties have increased from 30% to 40% since the COVID-19 pandemic among the general population.96–98 Moreover, this increase has been nearly two-fold among individuals with chronic conditions99,100 which may be explained by higher rates of mental illness and stress during the COVID-19 pandemic, which could provoke cognitive arousal and lead to sleep disruptions.101
Additionally, social distancing and quarantine mandates have led to a greater proportion of individuals with chronic conditions feeling lonely or socially isolated, which has been bidirectionally associated with disrupted sleep patterns.102 Further, atypical daily routines, sleep-wake times, meal and activity patterns, and often reduced light exposure may have led to the dysregulation of circadian rhythms, levels of arousal, and sleep drive in patients with chronic diseases.103
Despite the disruptions, many jobs and activities have transitioned into being completed at-home or remotely, thus offering more flexible schedules, and subsequently, the opportunity for patients to re-align their regular sleep-wake schedules to better fit their chronotypes and to better adhere to chronic illness management strategies.101
Treatment with positive airway treatment devices (PAP) for individuals with sleep-disordered breathing can be challenging during the COVID-19 pandemic because of PAP-induced droplets and aerosol, which act as mediums to transmit or spread the virus (SARS-CoV-2).104 Despite this, among obstructive sleep apnea (OSA) patients, compliance with continuous positive airway pressure (CPAP) therapy increased by 27% during the quarantine.105
Sleep health education must be prioritized as part of chronic disease management to promote better sleep quality and quantity for individuals with chronic conditions to prevent exacerbation of their conditions, which may be delivered through existing telemedicine channels.103
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7894869/
More information: Meghan O’Hearn et al. Coronavirus Disease 2019 Hospitalizations Attributable to Cardiometabolic Conditions in the United States: A Comparative Risk Assessment Analysis, Journal of the American Heart Association (2021). DOI: 10.1161/JAHA.120.019259



{kind=link}
[…] COVID-19: two-thirds of hospitalizations are due to four conditions – obesity… […]