









 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



Among the many startling images of the early coronavirus pandemic were the luxury cruise ships that garnered the nickname “floating incubators.”
No situation was more riveting than the ill-fated Diamond Princess, a British-registered ship that primarily cruises throughout Asia. The vessel’s storied—and deadly—quarantine at sea, which lasted nearly a month from February through early March of 2020, is helping environmental scientists shed new light on the dynamics of aerosol viral transmission.
New modeling research published in the Proceedings of the National Academy of Sciences, illustrates not only how SARS-CoV-2 likely spread among passengers and crew, but how the Diamond Princess may serve as an object lesson for other built environments and airborne viruses.
Environmental health investigators at Harvard University’s T.H. Chan School of Public Health and their collaborators have demonstrated that airborne transmission accounted for more than 50 percent of the disease spread aboard the cruise ship. Inhalation of virus-laden aerosols by passengers and crew occurred during close contact and at longer range, the scientists found.
Writing in the PNAS, Drs. Parham Azimi, Joseph G. Allen and colleagues underscore that it wasn’t aerosols alone that fueled a SARS-CoV-2 outbreak that affected hundreds aboard the luxury liner. Other routes of transmission contributed to the contagion, including fomite transmission, the spread of infection through contact with contaminated objects.
Their computational assessment of transmission pathways lends new insight into an outbreak in which 712 of the 3711 passengers and crew became infected, and more than a dozen died. Beyond the Harvard team’s assessment of how people aboard the Diamond Princess became infected, the new research tackles key concerns at the core of the ongoing pandemic—about droplets, aerosols as well as close contact and long-range infection.
One of the biggest concerns throughout the pandemic has centered on this question: What constitutes the most common mode of SARS-CoV-2 transmission?
The U.S. Centers for Disease Control and Prevention “has updated its position multiple times and currently underscores that SARS-CoV-2 is thought to spread mainly through close contact from person-to-person” (which the CDC defines as within 1.8 meters, or approximately six feet), Azimi and his colleagues wrote.
The agency, meanwhile, has been lukewarm about fomite transmission and the inhalation of respiratory droplets. Those methods of disease conveyance are likely not the primary ways the virus spreads, according to the CDC.
“It is important to note that there has been an argument about the size of these infectious aerosols and the range that they transmit,” Azimi told Medical Xpress.
“While the World Health Organization generally considers these particles to be less than 5 micrometers in diameter, aerosol scientists believe particles up to 10 micrometers in diameter or even larger can easily transmit within an indoor environment by small airflows mixing [with] the indoor air, interzonal or mechanisms such as an HVAC system’s [air] recirculation,” Azimi said, referring to a heating, ventilation and air conditioning system.
To evaluate the importance of multiple transmission routes of SARS-CoV-2 aboard the cruise ship, the team developed a modeling framework that utilized reams of detailed information from the Diamond Princess outbreak.
The Harvard environmental health scientists modeled 21,600 scenarios “to generate a matrix of solutions across a full range of assumptions for eight unknown or uncertain epidemic and mechanistic transmission factors,” they wrote in PNAS.
Aerosols smaller than approximately 10 micrometers, which were likely involved in all three modes of transmission – short- long-range and fomite transmission—likely contributed to more than half of the overall disease spread aboard the ship. Both large droplets and small aerosols contributed equally to transmission before passengers were quarantined, while small aerosols dominated transmission afterward.
The new Harvard findings underscore the importance of instituting measures to control small aerosol inhalation along with measures to control large droplet and fomite transmission. The authors emphasize that similar methods of assessment can be applied to the study of disease transmission risk in other built environments and for other airborne infectious diseases.
The Diamond Princess, as it turns out, was no stranger to disease outbreaks. It had been the site of a major norovirus epidemic in 2016. But gastroenteritis and a pandemic respiratory virus are completely different types of infection requiring different disease-control considerations.
When SARS-CoV-2 erupted, the rapid spread of infection to hundreds of passengers became a seafaring nightmare. No port would allow the vessel to dock for weeks. Passengers hailed from around the globe: Australia, Britain, Canada, India, Malaysia, the United States, and several other countries.
It was reported that the outbreak probably was ignited by a lone 80-year-old passenger from Hong Kong who had disembarked in January but had sowed the seeds of contagion while still on board.
The new research by the Harvard team adds new context to a CDC investigation that was conducted aboard the Diamond Princess a few weeks after it docked and passengers had disembarked. CDC scientists clad in hazmat suits boarded the star-crossed vessel and took biological samples as part of their outbreak assessment.
There was extensive evidence of SARS-CoV-2 RNA throughout passenger cabins, in hallways and other areas of the massive cruise liner. The inescapable presence of coronavirus RNA suggested explosive spread throughout the ship.
As part of their modeling research, Azimi and his colleagues relied on the Markov Chain Model, which uses “a discrete-time, discrete-space Markov chain” to estimate the number of SARS-CoV-2 copies present in numerous physical states, as well as the probability of transmission of SARS-CoV-2.”
“We chose the Markov Chain model over other existing infection transmission risk models because of its ability to stochastically track all modes of transmission under a wide variety of assumptions and with high computational efficiency. This approach offers advantages over the extensively used Wells-Riley model for quantitative infection risk assessment of respiratory infectious diseases in indoor environments, which does not consider all disease transmission routes,” the scientists wrote in PNAS.
Yet as detailed as their modeling study is – and it is possibly the most extensive and exhaustive of the Diamond Princess outbreak to date – there are still important questions that have yet to be answered. For one, how long do viral particles remain viable aerially?
“That is one of the biological factors that is very uncertain,” Azimi said. “In one of the most widely cited articles about the viability of SARS-CoV-2 [by virologist Neeltje van Doremalen of the National Institute of Allergy and Infectious Diseases] it is estimated that the half-life of SARS-CoV-2 in the air is approximately one hour.
This means that it would take about one hour for half of the infectious viruses to lose their viability. After two hours, 75 percent of viruses would lose their viability in indoor air, and so on.”
The modeling research by the Harvard-led team emphasizes that fomite transmission apparently played a role on the ship, albeit much smaller than aerosol spread. However, that finding suggests fomite transmission should not be shunted aside as possible risk factor.
“Although the contribution of fomite transmission is low it is still plausible, Azimi said. “It is important to notice that when we use our best estimates of model inputs, calculated from our PNAS paper, in other environments, such as school classrooms, the contribution of fomite transmission is about 5 percent. This contribution is low but it is not zero. Therefore, we do not recommend that people stop washing their hands.”
Shedding of SARS-CoV-2
Understanding viral shedding is important to optimize the treatment and prevent transmission. The reverse transcription polymerase chain reaction (RT-PCR) assays of SARS-CoV-2 RNA have been extensively used to demonstrate the presence of the virus due to its high sensitivity.
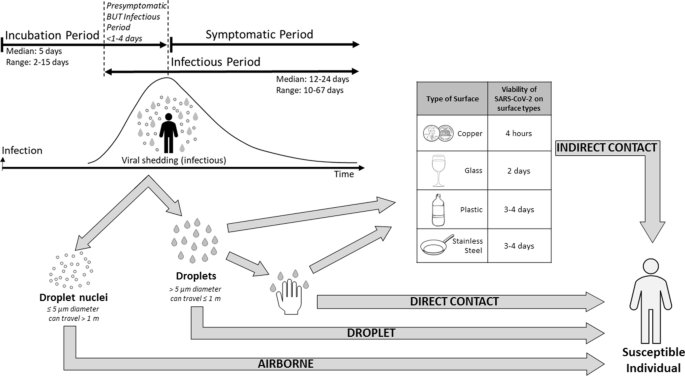
The studies found SARS-CoV-2 in respiratory samples, saliva, blood, feces, and rarely from urine (Pan et al. 2020; The COVID-19 Investigation Team 2020; To et al. 2020; Zheng et al. 2020; Zou et al. 2020). SARS-CoV-2 was detected from the pre-symptomatic period (Pan et al. 2020) and lasted significantly after symptom resolution (Fig. 2) (Dou et al. 2020; Lan et al. 2020; Li et al. 2020).
The median duration of viral shedding in respiratory samples was 12–24 days (Gombar et al. 2020; Hu et al. 2020a; Lo et al. 2020; Qi et al. 2020; Qian et al. 2020a; The COVID-19 Investigation Team 2020; Xiao et al. 2020b; Xu et al. 2020; Zheng et al. 2020; Zhou et al. 2020a). The longest reported duration was 67 days (Perera et al. 2020).
Duration of the virus in the respiratory samples was significantly longer in patients with severe disease (median 21 days, 14–30 days) compared to patients with milder disease (14 days, 10–21 days; P = 0.04) (Zheng et al. 2020). Among patients with severe symptoms, the duration of the viral shedding was significantly longer in male patients (Xu et al. 2020; Zheng et al. 2020), older age (Xiao et al. 2020a, 2020b; Xu et al. 2020; Zheng et al. 2020), and in patients on glucocorticoids treatment (Xu et al. 2020; Zheng et al. 2020), with longer time from symptom onset to hospital admission (Qi et al. 2020; Xu et al. 2020).
Significantly, the detection of viral RNA does not necessarily equate to infectious viruses being present (Atkinson and Peterson 2020). Presence of infectious viruses can be undoubtedly confirmed by cell culture, but it is difficult and expensive. Live virus isolation from throat swabs provide evidence of the virus replication in the upper respiratory tract (Bullard et al. 2020; Perera et al. 2020; Wolfel et al. 2020).
To distinguish viable virus from non-viable virus using PCR, RT-PCR tests for subgenomic mRNA can be applied. Viral subgenomic mRNA indicates the presence of actively infected cells in samples since subgenomic RNA is transcribed only in infected cells and is not present in virions (Kim et al. 2020).
The subgenomic mRNA of SARS-CoV-2 was detected in the upper respiratory samples and this indicates that active replication of SARS-CoV-2 occurs in the upper respiratory tract (Doddapaneni et al. 2020; Perera et al. 2020; Wolfel et al. 2020), whereas replication of SARS-CoV-1 mainly occurs in the lower respiratory tract (Cheng et al. 2004).
The replication in the upper respiratory tract makes SARS-CoV-2 more transmissible. The live SARS-CoV-2 was isolated during the first week of symptoms from swabs and sputum samples while no live SARS-CoV-2 was detected 8 days after symptom onset (Bullard et al. 2020; He et al. 2020; Perera et al. 2020; Sun et al. 2020; Wolfel et al. 2020). The subgenomic mRNA of SARS-CoV-2 was also detected up to 8 days after the onset of symptoms (Perera et al. 2020).
The high viral load in respiratory samples was observed at the time of symptom onset, but, viral loads gradually decreased during the disease progression (He et al. 2020; To et al. 2020; Wolfel et al. 2020; Zheng et al. 2020; Zou et al. 2020). Overall, high (> 1 × 106 copies per mL) viral load was detected from early days of infection (Pan et al. 2020).
The viral load in respiratory samples continued to be high during the third and fourth weeks after disease onset in patients with severe disease but the viral load was reduced after the second week in patients with mild disease (Zheng et al. 2020). Temporal profile of viral load corresponded well to the dynamics of SARS-CoV-2 infectiousness.
The infectiousness of SARS-CoV-2 starts from 1 to 4 days before symptom onset (Byrne et al. 2020) and peaked at 2 days before to 1 day after symptom onset and declined within 7 days (He et al. 2020). The median incubation period of COVID-19 is estimated to be 5 days with the 95% range spanning from 2 to 14 days (Linton et al. 2020).
The long incubation period and the high infectivity of SARS-CoV-2 during the incubation period make implementing the preventive measure difficult. Proportion of pre-symptomatic transmission was estimated to be 37–48% of transmission (He et al. 2020).
Furthermore, a significant portion of infected persons show no symptom but could still shed viruses (Zhou et al. 2020c). Asymptomatic infections were estimated at 15–30% (Chen et al. 2020; Long et al. 2020; Mizumoto et al. 2020; Nishiura et al. 2020).
However, asymptomatic infection may be more common than the current estimation. In Vo’, Italy, 43 percent of surveyed town residents tested positive despite having no symptoms (Lavezzo et al. 2020). Furthermore, when all passengers and crew were COVID-19 tested in a cruise ship, 80% of the COVID-19-positive patients were asymptomatic (Ing et al. 2020).
A recent review indicated that the asymptomatic patients could account for up to 45% of infections (Oran and Topol 2020). Viral transmission by asymptomatic carriers has also been reported in many studies (Bai et al. 2020; Hu et al. 2020c; Lavezzo et al. 2020; Qian et al. 2020b; Rothe et al. 2020; Tong et al. 2020).
Some investigations indicate transmission rates by asymptomatic patients are as high as symptomatic patients (Chen et al. 2020; Yin and Jin 2020) while others estimate the rate as one third of that of symptomatic transmissions (Wu 2020).
Indeed, there is no significant difference in viral load between asymptomatic and symptomatic groups (Zou et al. 2020) while the asymptomatic group shed virus significantly longer than the symptomatic group (Long et al. 2020). Those results indicate that the symptom-based screening is not enough to control transmission.
SARS-CoV-2 was also detected from stool (53–59%) and serum (40–59%) in a significant fraction of patients (Lo et al. 2020; Pan et al. 2020; To et al. 2020; Wang et al. 2020; Wolfel et al. 2020; Zhang et al. 2020b; Zheng et al. 2020). The positive rates for stool and serum samples gradually increased during the first week and decreased from the third week onwards (Zheng et al. 2020).
The live virus has been isolated from stool samples (Wolfel et al. 2020; Xiao et al. 2020c). Very few critically ill patients have detectable virus RNA in their urine samples (Zheng et al. 2020). The viral load of stool samples peaked during the third and fourth week after disease onset (Zheng et al. 2020).
The median duration of viral shedding in the stool samples was significantly longer than from respiratory and serum samples; 22 days (interquartile range 17–31 days) in stool, 18 days (interquartile range 13–29 days) in respiratory, and 16 days (interquartile range 11–21 days) in serum (Zheng et al. 2020).
Environmental contamination of SARS-CoV-2
Patients can be either pre-symptomatic, symptomatic, pauci-symptomatic, and asymptomatic shedding viruses in their vicinity. Environmental contamination in occupied patient rooms is known to be higher in the first week of illness for COVID-19 patients than the subsequent period of their stay due to high viral shedding. Persistence of viruses on the surfaces for a few days may promote transmission from these surfaces to healthcare workers (HCWs) to other patients. In addition, patients often share common spaces, therefore fomites can spread through touch contamination followed by self-inoculation of the mucous membranes.
The results of transmissibility of coronaviruses from contaminated surfaces in hospital settings are now emerging. Previous large outbreaks of MERS and SARS-CoV-1 have similarly been driven by the nosocomial spread. These studies confirmed that the environmental contamination is common. Some common themes have emerged from recent studies of hospitalized COVID-19 patients in several countries including China, England and Italy (Li et al. 2020; Razzini et al. 2020; Zhou et al. 2020b).
High-touch surfaces of hospitals are likely to be more contaminated than the low-touch surfaces (Tan et al. 2020). Moreover, within the hospital, intensive care units (ICUs) have the highest positivity of viruses, followed by isolation wards. A very little viral RNA was recovered from other areas of the hospital such as common areas, nursing stations, corridors, and anterooms.
Patients with severe COVID-19 symptoms tend to spread more viruses around them versus patients with milder symptoms. Interestingly, asymptomatic patients have been found to shed viruses in the environment which can also lead to further spread. In most studies, viable viruses have not been recorded (Wei et al. 2020).
The lack of viable viruses may be due to desiccation and death of the viruses at the time of collection. However, one study was able to recover viable viruses thus far. As mentioned earlier, transiently contaminated hands of healthcare workers are likely to have important implications for the viral spread.
Other areas include floors around bathroom toilets where the presence of viral RNA have been reported. Therefore, adherence to strict environmental cleaning policies is needed and routine hospital surface disinfection methods have been shown to decrease the presence of viruses on contaminated surfaces efficiently (Ryu et al. 2020).
In fact, one study depicts environmental sampling done after cleaning tested negative with no viral particles being recovered, whereas, if done prior to cleaning it yielded positive results with recovery of viral RNA (Hu et al. 2020b). In addition, higher viral load in patients corresponds to higher positivity rates of recovery of viral RNA from surfaces.
Fecal matter/stool samples from the toilet bowl, sink and door handles were found to be positive for SARS-CoV-2 by the PCR technique. Two possible contamination routes include either respiratory droplets contaminating the toilet or environmental fecal contamination.
The fecal contamination, caused by an infected person, also caused the spread of the SARS-CoV-2 virus (Zhang et al. 2020a). There is a possibility that larger outbreak can happen from viral stool shedding that can lead to sewage contamination. These findings contrast earlier reports by the WHO, which did not support the fecal–oral transmission of the SARS-CoV-2 virus (World Health Organization 2020b).
Survival of SARS-CoV-2 on healthcare surfaces
The indirect modes of transmission of coronaviruses through surface contamination/fomites have been controversial. Recent evidences suggest that most viruses such as coronaviruses, coxsackieviruses, influenza virus, MERS, and rhinoviruses can be present on the surfaces for prolonged periods of time. The fact that these viruses can survive for prolonged periods of time on different surfaces suggest that they can serve as possible reservoirs for onward transmission from surfaces to human (Kramer et al. 2006).
The duration that coronaviruses (SARS-CoV-1, MERS, SARS-CoV-2) persist on surfaces has been studied in vitro over the years (Chan et al. 2011; Coulliette et al. 2013; van Doremalen et al. 2020). Different surfaces made of plastics and metals demonstrated variable viral survivability. Typically, the type of test material has an influence on the survival of the viruses depending on their porosity.
A comparison of survivability of the coronaviruses on different types of dry surfaces is included as a table (Table 1). In general, survival of these viruses on plastic is longer than on steel. Interestingly, survival times for coronaviruses on copper surfaces have been consistently found to be the shortest, suggesting copper surfaces may be beneficial in preventing transmission (Noyce et al. 2007).
Other experimental factors that have been shown to influence virus viability in vitro include longer persistence of the viruses with higher inoculum, in presence of protein, serum, sputum or without dust (Casanova et al. 2010; Rabenau et al. 2005).
Lower temperatures improved survival of these viruses. Relative humidity is also an important factor that contributes to the virus survival. There have been reports of strain variation on survivability of influenza viruses, but this is largely unknown for coronaviruses (Coulliette et al. 2013; Dublineau et al. 2011).
Table 1 Persistence of coronaviruses on commonly used hospital surfaces under different environmental conditions
| Type of surface | HCoV-229E | SARS-CoV-1 | MERS-CoV | SARS-CoV-2 |
|---|---|---|---|---|
| Plastic | 2 d, 5 d Rabenau et al. (2005) Warnes et al. (2015) | 6 d, 4 d, 3 d, 28 d, 1 d Duan et al. (2003) van Doremalen et al. (2020) Chan et al. (2011) | 2 d, 8 h, 1 d van Doremalen et al. (2013) van Doremalen et al. (2020) | 3 d, 4 d van Doremalen et al. (2020) Chin et al. (2020) |
| Stainless steel | 5 d Warnes et al. (2015) | 2 d van Doremalen et al. (2020) | 8 h, 1 d, 2 d van Doremalen et al. (2013) | 3 d, 4 d van Doremalen et al. (2013) Chin et al. (2020) |
| Copper | 20 min, 30 min, 1 h Warnes et al. (2015) | 8 h van Doremalen et al. (2020) | – | 4 h van Doremalen et al. (2020) |
| Glass | 5 d Warnes et al. (2015) | 4 d Duan et al. (2003) | – | 2 d Chin et al. (2020) |
| Aluminum | 2 h, 6 h Sizun et al. (2000) | – | – | – |
| Brass | 10 min, 15 min, 2 h Warnes et al. (2015) | – | – | – |
Several methods have been employed to detect the presence of coronaviruses on various surfaces. The vast majority of the studies to date have used real-time PCR assays that can detect the virus as well as determine the viral load (Zuo et al. 2013). However, whether the virus is viable is not known when using this method (PCR).
Cell culture methods are usually used to detect the presence of viable viruses. It is of paramount importance to determine the infectivity of each virus because the mere presence of the viral RNA on a surface does not signify that they can be transmitted and infect another person.
Several other newer methods using CRISPR (Dara and Talebzadeh 2020) based diagnostic assays and loop mediated isothermal amplification (Lu et al. 2020; Yan et al. 2020; Yu et al. 2020) are also being applied for detecting the virus. Future studies on persistence of coronaviruses outside of its host are needed to define the role of contaminated surfaces on the transmission like those observed in cases of influenza and parainfluenza viruses.
Transmission characteristics of surface-to-person transmission
Larger droplets deposited onto surfaces via gravitational sedimentation occur relatively close to the emitter. This is likely a common contamination route for items within 2–6 m distance from the individual who coughs or sneezes (Xie et al. 2007). However, aerosolized particles less than 5 µm can also deposit on surfaces.
Mathematical models, based on information from studies taking sputum and swab samples, suggest that the typical emitter who is asymptomatic may emit enough virus through normal breathing to produce a concentration of 0.0043 copies/m3 of virus in a room with a normal air exchange rate or 0.000758 copies/m3 in a room with similar air exchange rate as a hospital (Lopez et al. 2013).
Under the same scenarios, they estimated that a high emitter may emit enough virus through normal breathing such that the concentration in a room is 560 copies/m and in a hospital room is 99 copies/m3. Frequent coughing from this high emitter boosts the estimate to more than 588,000 copies/m3 in a hospital room.
While this potentially poses risk of airborne transmission to anyone in the room as these particles remain suspended for long periods of time, some also settle onto surfaces, contaminating the surface. Thus, surfaces can be contaminated both by droplets and small aerosolized microdroplets.
Surfaces may also be contaminated via direct contact from the person to the surface. Julian et al. studied the transfer fraction ((f = Rr/(Rr + Rd) where Rr is the recipient surface and Rd is the donor surface) for 3 different phages to determine the transfer efficiency of the phages from a person’s skin to glass and vice versa (Julian et al. 2010). Using high and low inoculated surfaces of between 100 and 600 or 1000 and 6000 PFU in 5 µl, and allowed to dry, they determined the overall mean transfer fraction for all three phages combined was 0.23 with a standard deviation of 0.20.
Results from similar experiments that loaded much greater (1011 pfu) amounts of MS2 phage gave similar results as the above study under low relative humidity for transfer from fomite to finger for glass (19.3% (13.2%)), and in addition, they looked at a variety of surface types and humidity to understand how these factors might change the transfer efficiency (Julian et al. 2010).
Under high relative humidity, the transfer increased to 67.3% (25.0%). The transfer also varied greatly with the type of fomite. Under low humidity, acrylic (21.7% (15.0%)) and glass (19.3% (13.2%)) had greater transfer efficiency than other non-porous surfaces like ceramic tile (7.1% (4%)), laminate (5.4% (3.6%)), stainless steel (6.9% (8.9%)), and granite (10.2% (5%)).
Porous surfaces had very low transfer efficiencies with cotton (0.03% (0.02%)), polyester (0.3% (0.2%)), and paper currency (0.4% (0.4%)) all being similar. Under high humidity, the transfer efficiency increased across all materials except for cotton, with little effect on the porous surfaces, but large increases on the non-porous surfaces with acrylic (79.5% (21.2%)), glass (67.3% (25%)), ceramic tile (41.2% (18.8%)), laminate (63.5% (24%)), stainless steel (37.4% (16%)), and granite (30% (24.3%)) all showing marked increases in transfer efficiency.
In a more real-world approach, Rusin et al. showed that participants performing tasks (such as turning the faucet on/off and holding a phone receiver) that involved inoculated objects showed the highest transfer efficiencies for the phage from hard surfaces (faucet 33% and phone receiver 66%) (Rusin et al. 2002). The same study also showed 34% transfer efficiency of phage from inoculated fingertip to lip. Thus, contamination of surfaces via direct contact is very probable, especially for high-touch surfaces.
So-called high-touch surfaces have been described by several studies (Jinadatha et al. 2017; John et al. 2017). Certain surfaces, particularly bed-parts such as bedrails, receive a large amount of contact both by the patient and the healthcare workers. Touches to a surface generally do not occur in isolation, but rather as part of a sequence of touches involving a variety of fomites.
For example, when studying touch sequences of healthcare workers, a sequence could be defined as all of the touches a healthcare worker performs between their entry into a patient room and their exit (Jinadatha et al. 2017). During this time period, they may touch more than a dozen items in the room. Within these long sequences are sub-sequences of touches that occur more frequently.
For example, Jinadatha et al. reported that the most common sub-sequence within a patient care sequence was touching the patient and then the bedrail (28.1% of all patient care sequences contained this sub-sequence) or touching the bedrail and then the patient (26.3% of all patient care sequences contained this sub-sequence) (Jinadatha et al. 2017).
Touching a computer-on-wheels portable medical device and then the patient was the 5th most common sub-sequence. These findings demonstrate how interrelated all the items are in a room in terms of touch contacts. Given a certain probability to transfer a pathogen from a hand to a surface (as described in the transfer efficiency studies above), then it is possible that pathogens could be transferred to a surface and then to the patient or to another surface and then the patient.
If the fomite is a portable medical equipment (PME), then it may be brought into multiple patient rooms where the sequence of touches involves touching the portable medical equipment and then the patient or a surface that the patient may later touch.
As an oversimplified example, imagine a situation where a healthcare worker touched a contaminated fomite that contained 1,000 COVID-19 virus, subsequently touched a patient bedrail, and then the patient touched the same bedrail. Using a point estimated mean transfer efficiency of 0.23, 1000 * 0.23 (to healthcare worker hand) * 0.23 (healthcare worker to patient bedrail) * 0.23 (bedrail to patient hand) = 12 virus on the patient’s hand.
This oversimplified example, of course, makes many assumptions, particularly that the virus contact spot was touched completely on each subsequent surface and that the transfer efficiency was exactly 0.23 at each transfer. Even so, it is not hard to imagine the possibility of multiple fomites being contaminated in sequence via a variety of vectors.
The studies detailed above reveal large standard deviations in the reported transfer efficiencies, so when this error is included and propagated through an example like the above, rather than just using a point estimated transfer efficiency, then it is quite possible to calculate anywhere from zero virus transferred to a rather large number.
Thus, based on the available data, estimating the transfer of virus through a series of transfer events would be speculative at best. However, these studies do reveal that transfer through a series of events is quite possible.
Indeed, sequences of contact events where a fraction of pathogen is transferred with each successive touch as described above likely explain the findings by multiple studies that have reported widespread contamination of objects in the patient room, common work areas, and on portable medical equipment in the hospital after inoculating a few surfaces with cauliflower mosaic virus DNA markers (John et al. 2017; Oelberg et al. 2000).
reference link: Alimohamadi Y, Taghdir M, Sepandi M (2020) Estimate of the basic reproduction number for COVID-19: a systematic review and meta-analysis. J Prev Med Public Health 53(3):151–157. https://doi.org/10.3961/jpmph.20.076
reference link: More information: Parham Azimi et al. Mechanistic transmission modeling of COVID-19 on the Diamond Princess cruise ship demonstrates the importance of aerosol transmission, Proceedings of the National Academy of Sciences (2021). DOI: 10.1073/pnas.2015482118



{kind=link}