










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



A researcher from the University of Lahore Pakistan has proposed that the drug aprepitant could be used to target the neurokinin-1 receptors to prevent COVID-19 cytokine storms.
Aprepitant is a medication used in the management and treatment of chemotherapy-induced nausea and vomiting (CINV) and postoperative nausea and vomiting (PONV). It is in the neurokinin-1 antagonist class of medications.
The researcher hypothesized that the neuropeptide substance P (SP) as a possible cause of the initiation of cytokine storm developed in COVID-19 infection and to suggest Neurokinin-1 Receptor (NK-1R) antagonist, Aprepitant, as a drug to be used for its treatment.
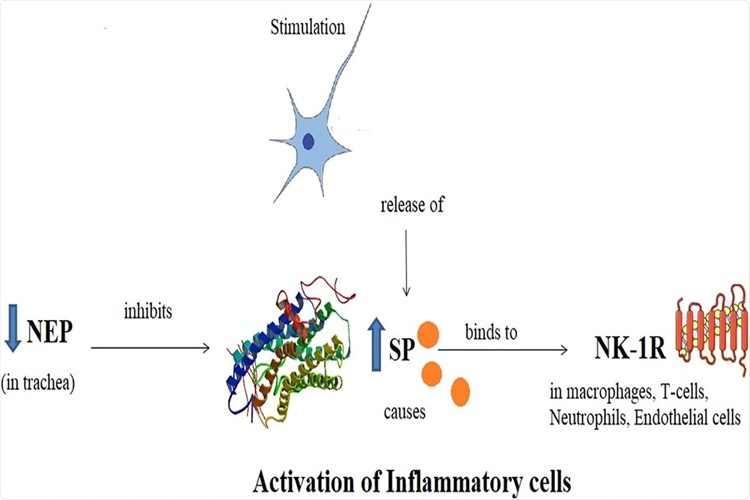
Schematic diagram showing Substance P, its receptor Neurokinin-1 and Neutral Endopeptidase. SP binds to NK-1R as a result of nociceptive stimulus and potentiates the inflammation. NEP acts as a regulatory mechanism by degrading the SP and hence, inflammation.
This proposed perspective will provide directions to the biomedical scientists to explore SP and NK-1R and prepare a drug to alleviate the symptoms and cure the disease.
It is very important to work on this perspective at earliest to reach to some conclusion regarding the therapeutic intervention. Clinical studies may also be conducted if proven successful.
It is responsible for the increased inflammation and the signature symptoms associated with this disease. It is the main switch that needs to be switched off by administering Aprepitant along with glucocorticosteroid, dexamethasone.
The opinion article was published in the peer reviewed journal: Biomedicine & Pharmacotherapy (Science Direct).
https://www.sciencedirect.com/science/article/pii/S0753332221009434
The SARS-CoV-2 coronavirus which cause the COVId-19 disease has a high transmission rate, and its symptoms may vary from being mild to severe pneumonia-like. Some individuals are also asymptomatically infected with the virus.
Common clinical manifestations of mild COVID-19 include cough, fever, muscular pain, loss of smell and taste, shortness of breath, vomiting, and sore throat. Severe infection may lead to organ failure, respiratory failure, and eventually death.
Researchers say that the novel coronavirus alone does not cause mortalityby itself rather the cytokine storm is responsible for respiratory failure, multiple organ failure, or heart attack that leads to death.
Researchers and scientists worldwide have been developing effective COVID-19 treatments. Several clinical trials are ongoing to evaluate various drugs with antiviral and anti-inflammatory effects.
This new opinion article propose s that Substance P (SP), via Neurokinin-1 Receptor (NK-1R), is responsible for the cytokine storm and inflammation in the case of severe COVID-19 infection.
The researcher aims to provide evidence that SP could be the possible factor for initiating the cytokine storm during severe SARS-CoV-2 infection. He has also proposed that such a condition could be effectively treated using Neurokinin-1 Receptor antagonist, aprepitant, as a potential therapeutic from the long list of prospective COVID-19 Drugs.
In 1931, Euler and Gaddum first discovered SP as a brain-gut hormone. https://physoc.onlinelibrary.wiley.com/doi/abs/10.1113/jphysiol.1931.sp002763
Subsequent extensive research revealed different roles of SP as a neuromodulator, neurotransmitter, and neurohormone, encoded by the gene named Tachykinin-1 (TAC-1).
Mechanisms by which SP-induced inflammation is implicated in the pathogenesis of COVID-19 infection. SP binds to NK-1R on endothelial cells to increase BBB permeability and release of cytokines by immune cells.
Furthermore it has been found that SP has many other functions, such as autocrine, paracrine, and endocrine functions. Scientists reported that SP and NK-1R are highly expressed in the central and peripheral nervous systems and the cardiovascular system. Immune cells such as leukocytes, lymphocytes, monocytes, and macrophages can also express SP.
Importantly SP is a chemokine that stimulates the cytokine release in respiratory tracts after attaching with NK-1R. These are also associated with various pathological conditions and inflammation.
Researchers have revealed that NK-1R is a 7-transmembrane domain, G-protein coupled receptor that possesses a high SP affinity.
Interestingly this receptor is also present in many cells such as white blood cells, lymphatics neurons, fibroblasts, vascular endothelium and, cardio-ventilatory regulatory centers. Previous research revealed that after the formation of the SP/NK1-R complex, a signaling cascade is responsible for the production of inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG).
It has been found that some of the early symptoms associated with COVID-19, such as cough, loss of smell and taste, headache, sore throat, are linked with the release of SP from trigeminal ganglion via TrN. Also, the release of the SP in the vagal C fibers in the larynx and upper respiratory tracts causes a cough.
Researchers have found that NK-1R antagonists could reduce the refractory cough frequency.
It has been also found that differential severity of SARS-CoV-2 infection in varied age groups are linked with the expression of SP. Mostly, SARS-CoV-2 is found to severely affect older age groups, compared to younger people. Many studies have indicated that the elderly tend to have elevated SP levels and that a higher concentration of SP leads to death.
Past research have revealed that individuals with co-morbidities such as diabetes mellitus (DM), hypertension (HTN), hepatic renal and cardiovascular conditions are more vulnerable to severe COVID-19 infection. Generally, patients with DM and HTN are treated with Dipeptidyl peptidase-4 (DPP4) and Angiotensin-converting enzyme (ACE) inhibitors. The spike proteins of the virus attach to the ACE2 of the host to establish infection.
Hence, ACE2 is the main receptor associated with SARS-CoV-2 infection, which is abundantly present in the lung capillaries, renal and endothelial cells of humans. A high level of SP dilates vessels, resulting in more blood pumping in the heart, thereby increasing the risks of a heart attack.
Increased levels of SP also lower the blood sugar level, causing multiple organ failure in severe COVID-19 cases.
Interestingly, previous research revealed that SP secretion by the immune cells is positively correlated with the viral load.
Numerous studies had indicated SP enhances inflammation via various mechanisms such as vasodilation and increased vascular permeability, leukocyte extravasation, and immune response activation in native cells and pathogens. In mice models, NK-1R deficient mice showed pulmonary inflammation as compared to controls.
Dr Riffat Mehboob, the author of this study strongly suggested that SP/NK-1R complex is associated with the pathogenesis of COVID-19 infection.
A combined therapeutic approach including corticosteroids, antibiotics, purified intravenous immunoglobulins and anti-cytokinic therapy should be recommended .
A recent randomized clinical trial associated with the evaluation of NK-1R antagonists (Dexamethasone and Aprepitant) for treating COVID-19 infection revealed that both the drugs showed improved clinical outcomes.
Also, patients who received the combination of these drugs reported improved clinical symptoms and reduced C-reactive protein. https://www.medrxiv.org/content/10.1101/2020.08.01.20166678v3
Substance P and Neurokinin-1 Receptor
SP was first discovered by V Euler and Gaddum in 1931 as a brain-gut hormone [6]. It is an undecapeptide which has role as neurotransmitter, neuromodulator and neurohormone, encoded by Tachykinin-1 gene (TAC-1) [7]. It is released from the fifth cranial nerve, the trigeminal nerve (TrN) and gives innervation to the orofacial region. SP and NK-1R are highly expressed in the enteric, central [8] and peripheral nervous system as well as cardiovascular system. It can also be expressed by immune cells such as leukocytes, lymphocytes, monocytes and macrophages [9], [10].
SP has autocrine, paracrine and endocrine functions and can affect the distant cells e.g. smooth muscle cells, fibroblasts, endothelial cells and muscle cells. It is a chemokine that regulates the immune and endocrine system and stimulates them to release cytokines in respiratory tracts after binding with NK-1R [11]. It is involved in several pathological conditions and inflammation [12].
NK-1R is a 7-transmembrane domain, G-protein coupled receptor with highest affinity for SP. Its full length form has 407 amino acids. It is present on many cell types in the body including the vascular endothelium and lymphatics, fibroblasts, white blood cells, neurons, cardio-ventilatory regulatory centers and phrenic nuclei controlling the diaphragm and respiration after binding to SP [7]. It is localized in brainstem nuclei controlling the rhythmic control [13]. SP/NK1-R complex, once formed, initiates a signaling cascade and produces inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG) [14]. Importantly, the macrophages and other immune cells produce inflammatory mediators by activation of NF-kB and releases the pro-inflammatory cytokines [15].
Evidence of possible involvement of substance P/ Neurokinin 1-Receptor in COVID-19 infection
Common orofacial symptoms in COVID-19 infection and SP nociception
Common and initial symptoms of COVID-19 infection includes sore throat, loss of sense of smell and taste, pain in eyes, headache and flue [3] and similar functions are carried out by SP once it is released from trigeminal ganglion via TrN. It provides somatosensory innervation to the orofacial region and has three branches: ophthalmic (V1), maxillary (V2) and mandibular (V3). So any alteration in its secretion in response to viral infection may result in symptoms in orofacial region [16] ( Fig. 1).

Schematic representation of Trigeminal nerve innervation in orofacial region. Noxious stimulus such as Corona virus enters through nose, mouth and eyes and reaches the trigeminal ganglion where it initiate the release of Substance P.
-> Involvement of SP in cough/airway hypersensitivity/asthma which are symptoms of COVID-19 infection as well
Vagal C fibers in larynx and upper airways secrete SP and cause cough. NK-1R antagonists are found to be helpful in reducing the refractory cough frequency [17], [18]. A study was conducted to assess the role of SP in clinical cough in humans. Serum SP levels were observed to be elevated in patients with persistent cough as compared to healthy controls. It was attributed to airway sensitivity in asthmatic cough [19].
-> Differential severity of COVID-19 infection in different age groups as addressed by the SP perspective
The mean age of COVID-19 patients was 45 years in a study conducted in China in which 161 patients were enrolled. Disease severity was found to be associated with older age [3] between 70 and 80 years and above [5]. So far, only few cases have been reported in children but with no complications, disease severity and deaths. In my previous studies related to sudden death [16], [20], I have reported that SP expression, if raised before birth may lead to fetal death, if decreased after birth may cause sudden infant death while in adults, higher SP expression may cause death [21]. Keeping this in view, higher SP may be fatal for older age groups which may be the case in COVID-19 patients. While children are found to be protective, because if SP is raised in them, they have no serious concerns.
-> SP/NK-1R theory addresses the high mortality rate in COVID-19 patients with hypertension, blood pressure and diabetes
Most affected patients with COVID-19 infection are observed to be those who already had co-morbidities such as hypertension (HTN), diabetes mellitus (DM), renal, hepatic and cardiovascular conditions [3], [22]. DM and HTN patients have increased risk of cardiovascular diseases. They use medicines such as Dipeptidyl peptidase-4 (DPP4) and Angiotensin-converting enzyme (ACE) inhibitors to reduce the cardiac conditions by vasodilating the vessels and lowering the blood pressure (BP) [23]. ACE is usually located in lung capillaries, renal and endothelial cells [24]. It may act as the receptor for SARS-COVID-19 [25]. SP also causes vasodilation. Elevated SP levels as a consequence of COVID-19 infection may further dilate the vessels, hence, more blood will be pumped by heart and more cardiovascular risk, leading to heart attack in complicated cases. It may also cause a lowering in BP, resulting in organ failure in severe cases [26]. It may explain, one of the possible underlying mechanism for mortalities due to COVID-19 infection.
-> Viral load correlates with the SP secretion
SP is secreted by the immune cells and is positively correlated with the viral load. SP may facilitate the replication of viruses by upregulation of CC Chemokine Receptor 5 (CCR5), necessary for HIV infection [15], [27]. If there is more infection, there will be more inflammation and elevated levels of SP. It can be used as a diagnostic and prognostic marker for COVID-19 infection.
-> SP initiates cytokine storming during inflammation-a possible mechanism in COVID-19 infection too
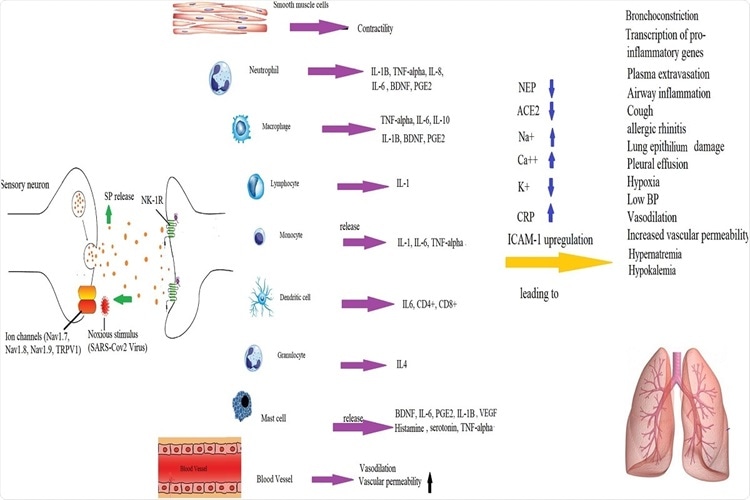
SP has immunomodulatory role and is an important link between nervous and immune systems [28]. SP initiates the release of all cytokines which in turn, further stimulates SP and the NK-1R [29]. SP boosts the inflammation in all three possible ways: First, by vasodilation and increasing the vascular permeability, Second, by leukocyte extravasation and third, by directly acting on native cells and the foreign invaders to activate their immune characteristics ( Fig. 2, Fig. 3) [30]. During inflammation, SP is secreted by immune system such as macrophages, dendritic cells, lymphocytes and neutrophils as well as other cells such as endothelial cells [11]. SP activates the immune cells to produce cytokines, chemokines and histamines by mast cells [31]. It inhibits the cytokine TGF-β1, which is an immune-suppressor, released by macrophages [32] and thus promotes inflammation. It also induces the proliferation of T-lymphocytes, B-lymphocytes and natural killer cells, resulting in immunoglobulin secretion [33]. IFN-γ and TNF-α can activate the upregulation of NK-1R in macrophages like IL-4 [34].

SP is the first to react in response to a noxious stimulus. It is a rapid, immediate defense and survival system. In experimental studies, NK-1R deficient mice exhibited reduced pulmonary inflammation as compared to controls [35]. The immune response prevents the host cells by fighting against the pathogen but if it continues uncontrolled, it may be fatal. This phenomenon is known as “cytokine storming” (Fig. 2, Fig. 3). Inflammatory mediators continue to be secreted by immune cells and can cause acute respiratory distress syndrome (ARDS) in COVID-19 infected patients. So, it is not actually the pathogen that is fatal, but the cytokine storming. If prevented or reversed, it may save the infected patients from further complications [36], [37].
Neutral Endopeptidase (NEP) reduces inflammation by degrading SP
NEP or ‘Enkephalinase’ degrades SP and reduces the inflammation in respiratory tracts and associated conditions such as cough, edema and bronchoconstriction. It is localized in nerves, smooth muscle, trachea, and epithelium. In a study conducted on rats with respiratory infections caused by rat corona virus, parainfluenza type virus 1 and Mycoplasma pulmonis, had greater inflammation, reduced NEP activity and higher SP as compared to the pathogen free rats. NEP modulates the functionalities of SP. Respiratory tract infections may increase the airways responsiveness, cause inflammation, leading to bronchoconstriction due to raised SP (graphical abstract) [38]. Hence, the respiratory tract infections may be treated by elevating the NEP by its agonists. This is another possible treatment strategy.
reference link : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8435369/



{kind=link}