











 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The TAG-VE was convened on 26 November 2021 to assess the SARS-CoV-2 variant: B.1.1.529.
The B.1.1.529 variant was first reported to WHO from South Africa on 24 November 2021. The epidemiological situation in South Africa has been characterized by three distinct peaks in reported cases, the latest of which was predominantly the Delta variant. In recent weeks, infections have increased steeply, coinciding with the detection of B.1.1.529 variant.
The first known confirmed B.1.1.529 infection was from a specimen collected on 9 November 2021.
This variant has a large number of mutations, some of which are concerning. Preliminary evidence suggests an increased risk of reinfection with this variant, as compared to other VOCs.
The number of cases of this variant appears to be increasing in almost all provinces in South Africa. Current SARS-CoV-2 PCR diagnostics continue to detect this variant.
Several labs have indicated that for one widely used PCR test, one of the three target genes is not detected (called S gene dropout or S gene target failure) and this test can therefore be used as marker for this variant, pending sequencing confirmation. Using this approach, this variant has been detected at faster rates than previous surges in infection, suggesting that this variant may have a growth advantage.
There are a number of studies underway and the TAG-VE will continue to evaluate this variant. WHO will communicate new findings with Member States and to the public as needed.

based on the data provided, there are the following reports of cases of contagion from COVID-19 variant B.1.1.529
Country Submission Count
| Country | Total #GR/484A (B.1.1.529) | #GR/484A (B.1.1.529) in past 4 weeks | %GR/484A (B.1.1.529) in past 4 weeks |
|---|---|---|---|
| South Africa | 110 | 110 | 71.0 |
| Botswana | 19 | 19 | 19.2 |
| Australia | 5 | 5 | 0.3 |
| Hong Kong | 3 | 3 | 12.0 |
| United Kingdom | 2 | 2 | 0.0 |
| Canada | 2 | 2 | 0.1 |
| Italy | 1 | 1 | 0.0 |
| Belgium | 1 | 1 | 0.1 |
| Israel | 1 | 1 | 0.1 |
| Austria | 1 | 1 | 0.5 |
Omicron Variant Characteristics
Mutation in Omicron Variant
- Omicron Variant was spotted in genome-sequencing data from Botswana.
- This variant contains more than 30 changes in the spike protein of the SARS-CoV-2 virus.
- Researchers in Rome shows 43 spike protein mutations.
| classification | Pangolin | WHO | Alternative name | First proof | Amino acid exchanges in the S protein |
|---|---|---|---|---|---|
| VOC | B.1.1.529 | Omicron | GR / 484A, 21K | Botswana, Nov 2021 | A67V, Δ69-70, T95I, G142D / Δ143-145, Δ211 / L212I, ins214EPE, G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493K, G8496S, N450K, G8496S, T547K, D614G, H655Y, N679K, P681H, N764K, D796Y, N856K, Q954H, N969K, L981F |



Mutations from the root (Source- NextStrain)
- 86 nucleotide mutations
- C241T, A2832G, C3037T, T5386G, G5924A, G6513-, T6514-, T6515-, G8393A, C10029T, C10449A, T11285-, T11286-, G11287-, T11288-, C11289-, T11290-, G11291-, G11292-, T11293-, A11537G, T13195C, C14408T, C15240T, A18163G, C21762T, T21765-, A21766-, C21767-, A21768-, T21769-, G21770-, C21846T, G21987-, T21988-, G21989-, T21990-, T21991-, T21992-, A21993-, T21994-, T21995-, A22194-, T22195-, T22196-, G22578A, T22673C, C22674T, T22679C, G22813T, T22882G, G22898A, C23202A, A23403G, C23525T, T23599G, C23604A, C23854A, G23948T, C24130A, A24424T, T24469A, C24503T, C25000T, C25584T, C26270T, A26530G, C26577G, G26709A, A27259C, C27527T, C27807T, A28271T, C28311T, G28362-, A28363-, G28364-, A28365-, A28366-, C28367-, G28368-, C28369-, A28370-, G28881A, G28882A, G28883C.
- Nextstrain clade- 21K
- GISAID clade- GR/484A
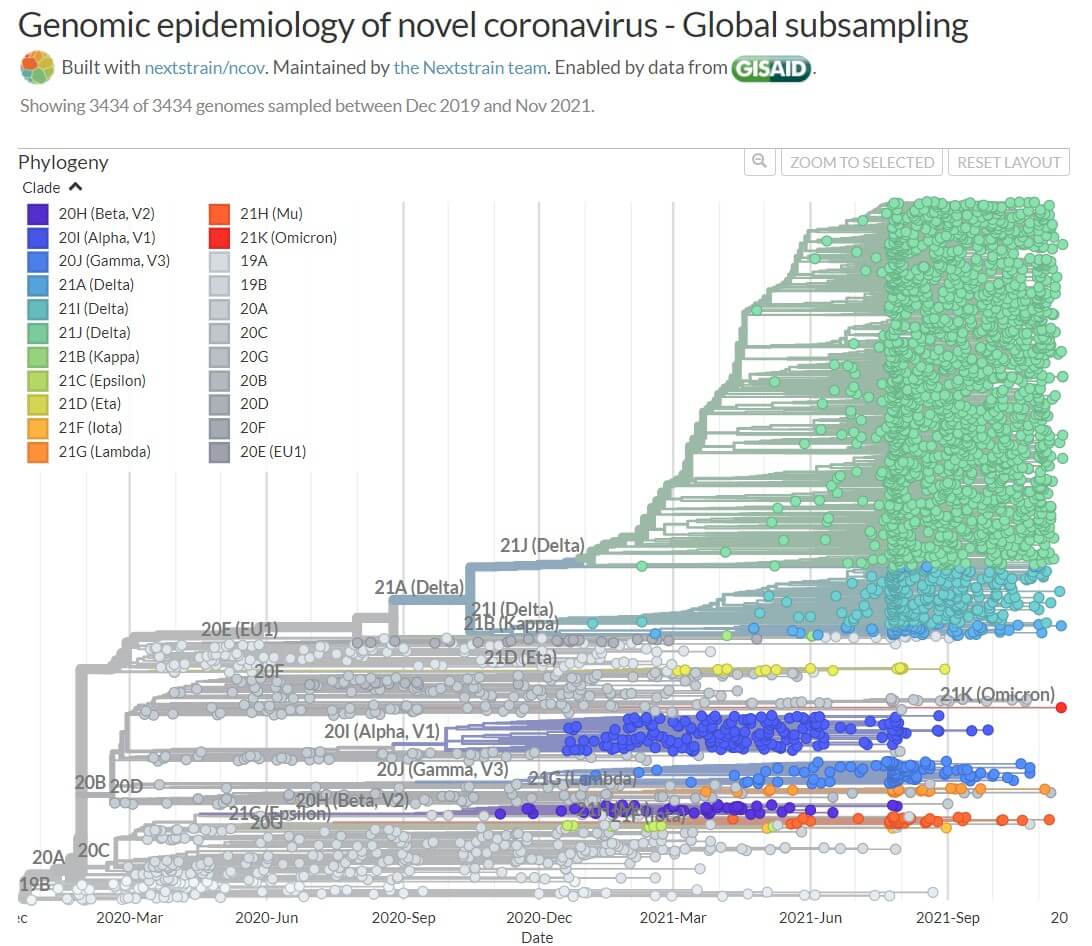
Figure: Position of Omicron Variant in Phylogeny. Image Source: NextStrain.
Living Evidence – SARS-CoV-2 variants
urrently, the World Health Organization has identified four variants of concern: Alpha, Beta, Gamma and Delta.
| Alpha (B.1.1.7) | Beta (B.1.351) | Gamma (P.1) | Delta (B.1.617.2) | Omicron (B.1.1.529) | |
|---|---|---|---|---|---|
| WHO label | Alpha | Beta | Gamma | Delta | Omicron |
| Scientific names | B.1.1.7GRY (formerly GR/501Y.V1)20I/S:501Y.V1 | B.1.351GH/501Y.V220H/S:501Y.V2 | B.1.1.28.1 (P.1)GR/501Y.V320J/S:501Y.V3 | B.1.617.2G/452.V321A/S:478K | B.1.1.529GR/484A |
| First detected | UKSeptember 2020 | South AfricaMay 2020 | BrazilNovember 2020 | IndiaOctober 2020 | Botswana, South Africa November 2021 |
| Mutations | 23 (17 of which change amino acids) Includes N501Y substitution | 21 (8 of which change amino acids)Includes N501Y substitution | 17 (11 of which change amino acids) Includes N501Y substitution | 12Includes spike mutation profiles L452R, E484Q and D614G and lacks mutations at amino acid positions 501 or 484 in its ACE2 receptor.Properties found in Delta that might account for its transmissibility: cells fuse more efficiently, faster and at lower levels of the receptor*^P681R change is a crucial feature of Delta*^Characterised by an excess of non-synonymous mutations,Sub-lineages are given the alias of AY. | 50 mutations, including over 30 mutations on its spike protein and 15 on the receptor binding domain |
| Transmissibility compared with wild type | Reproduction number (Ro) ~3.5-5.2*^Increased transmissibility and secondary attack rate compared with wild type*^Estimated 43–90% higher reproduction number than wild type and transmission advantage at warmer temperatures *^Estimated higher rates of transmission in children aged 0 to 9 years. Reports of high seroprevalence rate in secondary school-aged children*^ and some studies inferring an increase in within-school transmission*^ | Increased transmissibility and estimated to be 2.5 times greater than wild type*^ | Increased transmissibility and secondary attack rate compared with wild type^ | Reproduction number (Ro) ranges from 3.2 to 8, with a mean of 5.0.Increased transmissibility and secondary attack rate compared with wild type*^ for household and non-household contacts.Estimated 2.5-fold higher viral loads compared to other variants*^. Similar viral loads between vaccinated and unvaccinated individuals*^Virological characteristics of vaccine breakthrough infections suggest Ct-values decreased throughout the first three days of illness*^. Data from England suggests a doubling time of 25 days*^. Estimated mean of the latent period and the incubation period are 4.0 days and 5.8 days, respectively*^ | It is not yet clear whether Omicron is more transmissible*^News report (27 Nov 2021) of a surge of cases in South Africa a from 273 cases on 16 November to more than 1,200 by the start of this week. More than 80% of these were from Gauteng where the variant is the dominant strain. The R value is estimated to be 1.47 for South Africa, but 1.93 in Gauteng.^ |
| Virulence / severity or duration of disease / reinfection | Increased risk of hospitalisation, possible increased risk of severity and mortality*^Average infections last 13.3 days compared with 8.2 days for other variants*^ and Alpha does not appear to influence patient trajectories including onset to hospitalisation and length of stay*^ | Possible increased risk of severe disease and in-hospital mortality*^ | Possible increased risk of hospitalisation and severity of disease *^ | Increased risk of emergency care and hospitalisation, including higher odds of oxygen requirement, admission to an intensive care unit, and possible increased risk of mortality*^Studies show hospitalisation rates for unvaccinated individuals are higher compared with vaccinated individuals*^Summary of vaccine effectiveness against different outcomes: infection, symptomatic disease, hospitalisation and morality*^. Estimated vaccine effectiveness against hospitalisation and ICU admissions*^Estimated reinfection risk of ~46% *^. Prior infections result in less severe disease against subsequent infections*^Resistant against Bamlanivimab*^ and efficiently inhibited by Etesevimab, Imdevimab and by Casirivimab/Imdevimab*^Some studies suggest symptoms can differ to wild type*^.Reports that asymptomatic cases clear more quickly, 11 days compared to 1 day, and had higher mean antibody levels than symptomatic cases *^Estimated illness duration for children is 5 days, with symptoms including headache and fever*^. Reports of low hospital presentation and the presence of long illness*^ | It is not yet clear whether Omicron causes more severe disease, compared to infections with other variants, including Delta*^Preliminary data suggests increasing rates of hospitalisation in South Africa, but this may be due to overall increasing rates of infection*^Preliminary evidence suggests an increased risk of reinfection*^Currently no information to suggest symptoms differ to other variants*^ |
| Immune escape (vaccines / previous infections will not be protective) | |||||
| Comirnaty (Pfizer – BNT162b2) | Estimated <2-fold reduction in neutralisation*^Full vaccination (≥7 days after dose 2) up to 89% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile^* | Estimated 5 to <10-fold reduction in neutralisation*^Full vaccination (≥7 days after dose 2) up to 84% vaccine effectiveness against symptomatic infection*^Neutralisation increased with prior COVID-19 infection*^Vaccine effectiveness profile^* | Estimated 2 to <5-fold reduction in neutralisationFull vaccination (≥7 days after dose 2) up to 84% vaccine effectiveness against symptomatic infection*^Neutralisation increased with prior COVID-19 infection*^Vaccine effectiveness profile^* | Estimated 5 to <10-fold reduction in neutralisation with some studies suggesting an 11.30-fold reduction^*Full vaccination (≥7 days after dose 2) up to 87% vaccine effectiveness against symptomatic infection^*. Another study suggests ~90%, ~85% and 79% effectiveness after 30, 60 and 90 days respectively*^Vaccine effectiveness profile*^Reported drops in vaccine effectiveness*^ from multiple studies*^, however, there is evidence for the maintenance of protection against severe disease*^ including hospitalisation and mortality*^Reports suggest a strong effect of waning immunity*^Reports of phase 3 data show booster (third) dose induces significant neutralising antibody titers*^ with an estimated reduction in relative risk for confirmed infection and severe disease *^. Estimated to be ~95.6% effective*^. One study suggests vaccine effectiveness from 14 days after the booster was ~93.1% when the primary course was Vaxzevria (AstraZeneca) and ~94% for Comirnaty (Pfizer) against symptomatic disease*^ | Studies under way to understand the effectiveness of vaccinesBioNTech have said it could produce an updated vaccine within 100 days if the new variant is found to evade existing immunity.^ |
| Vaxzevria (AstraZeneca -ChAdOx1)) | Estimated 5 to <10-fold reduction in neutralisation*^Vaccination (≥14 days after dose 1 only) up to 64% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile^* | Estimated 5 to <10-fold reduction in neutralisation*^Vaccination (≥14 days after 1 dose only) up to 48% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile^* | Estimated 2 to <5-fold reduction in neutralisation*^Vaccination (≥14 days after dose 1 only) up to 48% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile | Estimated 2 to <5-fold reduction in neutralisation*^Vaccination (≥14 days after one dose only) up to 67% vaccine effectiveness against symptomatic infection*^. Another study suggests ~69% effectiveness after 14 days after the second dose, and 61% at 90 days*^Vaccine effectiveness profile*^Breakthrough infections may cause asymptomatic or mild disease, but are associated with high viral loads, prolonged PCR positivity and low levels of vaccine-induced neutralising antibodies*^Reported drops in vaccine effectiveness, however, there is evidence for the maintenance of protection against severe disease*^ | Studies under way to understand the effectiveness of vaccines |
| Spikevac (Moderna -mRNA-1273) | Estimated <2-fold reduction in neutralisation*^Full vaccination (≥7 days after dose 2) up to 92% vaccine effectiveness against symptomatic infection*^ Vaccine effectiveness profile^* | Estimated 5 to <10-fold reduction in neutralisation*^Vaccination (≥14 days after dose 1 only) up to 77% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile*^ | Estimated 2 to <5-fold reduction in neutralisation*^Vaccination (≥14 days after dose 1 only) up to 77% vaccine effectiveness against symptomatic infection*^Vaccine effectiveness profile*^ | Estimated 2 to <5-fold reduction in neutralisation*^Vaccination (≥14 days after dose 1 only) up to 72% vaccine effectiveness against symptomatic infection*^Reports that two-dose vaccine effectiveness was ~86.7% against Delta infection and ~97.6% against hospitalisation; however, declined with increasing time since vaccination*^Vaccine effectiveness profile^*Reported drops in vaccine effectiveness*^ However, there is evidence for the maintenance of protection against severe disease*^ | Studies under way to understand the effectiveness of vaccinesModerna have said they are working to advance a booster candidate tailored to the new variant and has been testing a higher dose of its existing booster.^ |
| Novavax (NVX-CoV2373) | Estimated <2-fold reduction in neutralisation*^Vaccine effectiveness profile^* | Estimated ≥10-fold reduction in neutralisation*^Vaccine effectiveness profile^* | Vaccine effectiveness profile*^ | Studies under way to understand the effectiveness of vaccines | |
| Johnson & Johnson (Ad26.COV2.S) | Estimated 2 to <5-fold reduction in neutralisation*^Vaccine effectiveness profile^* | Estimated ≥10-fold reduction in neutralisation*^Vaccine effectiveness profile^* | Estimated 2 to <5-fold reduction in neutralisation*^Vaccine effectiveness profile^* | Estimated <2-fold reduction in neutralisation^* Vaccine effectiveness profile*^ | Studies under way to understand the effectiveness of vaccines |
| Immune escape – other | Elicits cross-reactive neutralising antibodies*Sinovac-CoronaVac: significant reduction in neutralising antibody capacity compared to wild type*^Reports of breakthrough infections*^ | Elicits cross-reactive neutralising antibodies^Bharat-Covaxin (BBV152): neutralisation with an estimated 3-fold reduction*^Sinovac-CoronaVac: significant reduction in neutralising antibody capacity compared to wild type*^ | Elicits cross-reactive neutralising antibodies^Sinovac-CoronaVac: estimated <2-fold reduction in neutralisation and a reduction in vaccine effectiveness*^Cases of reinfection with an estimated 6.4% reinfection probability*^Neutralistion increased with prior COVID-19 | Transmission is associated with an escape to antibodies targeting non-RBD and RBD Spike epitopes*^Review of vaccine efficacy, effectiveness and neutralisation data for variants*^ | Preliminary data presented at an initial briefing hosted by South Africa’s Department of Health suggests some mutations may be associated with increased antibody resistance*^, and early reports from the UK Health Security Agency suggest the mutation profile may change how the virus behaviours with regards to immune escape and susceptibility to some treatments, particularly therapeutic monoclonal antibodies, however this is not yet confirmed*^ |
| Testing and detection | Limited impact.S gene target failure; no impact on the overall result from multiple target RT-PCR, no impact on Ag RDTs observed. | No impact on RT-PCR or Ag RDTs*^ | No reported impacts on diagnostics*^ | No reported impacts on diagnostics*^Lateral flow devices effective in detecting*^ and used as part of the asymptomatic testing program in the UKEstimated lower PCR Ct values and significantly longer duration of Ct value ≤30 (estimated median duration 18 days for Delta and 13 days for wild-type)*^ One study suggests higher loads do not translate into different testing scenarios*^ | No reported impacts on diagnostics*^ |
| Countries reporting detection (not necessarily local transmission) | Detected in ~174 countries | Detected in ~116 countries | Detected in ~74 countries | Detected in ~142 countriesCurrent global epidemiology can be characterised by a predominance of Delta.AY.4 is the dominant lineage in the UK, | Detected in NSW Australia and at least ~11 other countries: Botswana, South Africa, Belgium, Israel, Hong Kong, United Kingdom, Italy, Germany, Denmark, Netherlands, the Czech Republic^ |
The World Health Organization (WHO) announced the Variant naming system on 1 June 2021. The labels do not replace existing scientific names. Designations include Variant of Concern (VOC), Variant of Interest (VOI) and Variants Under Monitoring (VUMs). A previously designated VOC or VOI can also be reclassified if it no longer poses a major added risk to global public health.
Details are tabulated when Variants meet the World Health Organization (WHO) definition of Variant of Concern (VOC).
Reports of Variants of Interest (VOI) are updates identified in the grey literature are below:
- Variants of Interest VOI) listed by WHO: Lambda (C.37) and Mu (B.1.621).
- Variants Under Monitoring (VUMs) listed by WHO: former VOI Eta (B.1.525), Iota (B.1.526), Kappa (B.1.617.1) and other Pango lineages.
- The Mu variant (B.1.621) was marked as a VOI on 30 August 2021. This includes the descendent Pango lineage B.1.621.1. The Mu variant has a constellation of mutations that indicate potential properties of immune escape. First identified in Colombia in January 2021^*. Public Health England has published an initial risk assessment on Mu*^. Mutations in the receptor-binding domain of the spike protein may contribute to increased transmissibility*^. Reports of ineffective neutralisation by convalescent and vaccine sera*^. Reports suggest two mutations in the spike protein YY144-145TSN and E484K, are responsible for the potent immune resistance of Mu variant*^. Early reports that Comirnaty (Pfizer – BNT162b2) has 76% neutralizing effectiveness against the Mu*^, and ~90.4% two-dose effectiveness for Spikevac (Moderna -mRNA-1273*^. Another study suggests Mu were partially resistant to neutralising antibody, neutralising titers elicited by mRNA vaccination remained above what is found in convalescent sera and thus are likely to remain protective against severe disease*^.
- The Lambda variant (C.37) was marked as a VOI on 14 June 2021 and is associated with high rates of transmission in multiple countries. Lambda is characterised by mutations in the spike protein, including G75V, T76I, del247/253, L452Q, F490S, D614G and T859N with estimated increased infectivity and immune escape*^ Early studies suggest that vaccines in current use will remain protective against Lambda and that monoclonal antibody therapy will remain effective*^ Public Health England published a risk assessment on Lambda*^
- Delta-AY.2 (Delta with K417N) is being reported as ‘Delta Plus and ‘Delta +’. Information suggests that there are at least 2 separate clades of Delta with K417N. There is no clear evidence that ‘Delta Plus’ is more transmissible or immune evasive than Delta Variant, with some reports suggesting an increase in secondary attack rate and household transmission risk*^ for AY.4.2. Delta with K417N can be detected by genotyping assay. Biological data suggest that Delta with K417N is unlikely to show substantial antigenic change compared to Delta. A preliminary rapid vaccine effectiveness analysis does not suggest a significant reduction in vaccine effectiveness for AY.4.2 compared to Delta*^, preliminary viral neutralisation studies with post-vaccine sera show a 2.8 fold reduction in comparison to the wild type, similar to Delta*^. Delta sub-lineage AY.4.2 has been designated as a Variant Under Investigation by the UK Health Security Agency and has been given the official name VUI-21OCT-01 and it accounts for ~11.2% of all Delta cases in the UK*^.
- Technical briefing 26 was published by UK Health Security Agency on 26 November 2021.
1. Background
- On 26 November 2021, on the basis of advice from WHO’s Technical Advisory Group on Virus Evolution, WHO designated the SARS-CoV-2 variant B.1.1.529 a variant of concern (VOC). This variant has been given the name Omicron.
- The variant Omicron was first reported to WHO from South Africa on 24 November 2021. In recent weeks, infections have increased steeply in South Africa, coinciding with the detection of Omicron. The first known confirmed Omicron infection was from a specimen collected on 9 November 2021, and the first publicly available sequence from a specimen collected on 11 November 2021. The number of cases of this variant appears to be increasing in multiple provinces in South Africa.
- The variant Omicron was also detected in Botswana in samples collected on 11 November 2021. As of 28 November 2021 3pm, cases have been detected in several additional countries in four WHO regions. While most of the current cases in these countries are travel-related, we expect this to change as more information becomes available.
- Omicron has an unprecedented number of spike mutations, some of which are concerning for their potential impact on the trajectory of the pandemic. Preliminary evidence suggests there may be an increased risk of reinfection with this variant, as compared to other variants of concern (VOCs).
- Current SARS-CoV-2 PCR diagnostics are able to detect the Omicrom variant. Several labs have indicated that for one widely used PCR test (ThermoFisher TaqPath), one of the three target genes is not detected (called S gene dropout or S gene target failure, SGTF) and this test can therefore be used as marker for this variant, pending sequencing confirmation.
- Studies underway to evaluate the transmissibility, severity and reinfection risk of Omicron. Additional studies are needed to understand effectiveness of vaccination, by product, and by infection and disease outcomes. WHO will communicate new findings with Member States and to the public as this information becomes available.
2. Global risk assessment
- There is substantial uncertainty regarding Omicron’s transmissibility, immune escape potential (from either infection- or vaccine-induced immunity), clinical presentation, severity of disease, and response to other available countermeasures (e.g. diagnostics, therapeutics). A number of researchers in South Africa and other countries are carrying out studies to assess these characteristics of Omicron. Depending on these characteristics, if another major surge of COVID-19 takes place driven by Omicron, consequences may be severe. Increasing cases, regardless of a change in severity, may pose overwhelming demands on health care systems and may lead to increased morbidity and mortality. The impact on vulnerable populations would be substantial, particularly in countries with low vaccination coverage. To date, no deaths linked to Omicron variant have been reported.
- At present, local transmission has been reported in South Africa and there is evidence of spread to several countries in four WHO regions (African, Eastern Mediterranean, European, and Western Pacific regions). While most of the cases identified in these countries are travel-related, we expect this to change as more information becomes available.
- Overall risk related to the new variant of concern Omicron is thus considered very high. The evidence for this assessment contains considerable uncertainty and will be updated as more information becomes available.
3. Priority Actions for Member States
Based on the risk assessment, the following priority actions are recommended to enhance readiness for the new variant of concern Omicron.
3.1 Enhanced Surveillance
- Ensure early warning systems are in place, composed of multiple indicators such as rapid growth (e.g. growth rate, effective reproduction number), case incidence, and test positivity proportion. It is also crucial to monitor indicators related to disease severity and pressure on health care systems (e.g. bed occupancy of general ward and intensive care unit)
- Enhance event-based surveillance for unusual epidemiological signals:
- Reports of rapidly spreading outbreaks in healthcare facilities or communities might raise the concern that these events are due to a variant that spreads more easily from person to person.
- Similar reports from populations expected to have a high level of immunity (due to prior infections or high vaccination coverage) may indicate the presence of a variant able to evade the immune response.
- Outbreaks causing unexpectedly high levels of morbidity and mortality may be due to a variant causing more severe disease.
· Report initial cases/clusters associated with Omicron infection to WHO through the IHR mechanism.
- Thereafter, report (publicly or through IHR) the proportion of Omicron amongst sequenced samples (and/or, where available, the proportion of SGTF)
- Where capacity exists and in coordination with the international community, perform field investigations and laboratory assessments (see below) to improve understanding of transmission parameters, vaccine effectiveness, severity, effectiveness of public health and social measures against Omicron, diagnostic methods, immune responses, antibody neutralization, or other relevant characteristics. Specimens collected during such investigations may warrant prioritization for sequencing.
- When recording case data, particular attention should be paid to cases’ vaccination status and date of vaccination; history of previous SARS-CoV-2 infection; symptoms/clinical presentation; and clinical severity/outcome.
- The epidemiological studies and sequencing of specimens can be targeted to those with particular individual-level characteristics (e.g. suspected reinfections, clinical characteristics; immunocompromised patients and selective sequencing of vaccine breakthrough), as well as usual clusters and super-spreader events.
- For further details on surveillance in the context of emerging variants, including sampling strategy, please refer to WHO guidance for surveillance of SARS-CoV-2 variants Interim guidance 9 August 2021; additional guidance is available from ECDC Guidance for representative and targeted genomic SARS-CoV-2 monitoring.
3.2 Laboratory
- The variant of concern Omicron belongs to Pango lineage B.1.1.529, Nextstrain clade 21K, GISAID clade GR/484A, is characterized by 45-52 amino acid changes, including 26-32 the spike protein
compared to the reference strain.
- Most diagnostic tests continue to work and can detect the variant of concern Omicron.
- S gene dropout or S gene target failure (SGTF) due to deletion at Spike position 69-70, similar to the detection of the Alpha variant, has been reported. The ThermoFisher TaqPath assay can therefore be used as proxy test for this variant, pending sequencing confirmation. Use of the SGTF approach may lead to faster detection rates.
- Studies are ongoing to assess if some SARS-CoV-2 antigen-based rapid diagnostic tests (AgRDT) may be impacted by this variant.
- In countries with sequencing capacity, WHO advises that a representative subset of SARS-CoV-2 confirmed cases be sequenced. In addition to randomly selected samples to achieve representativeness, sampling selection criteria should include cases from any unusual transmission events (e.g., increased transmission despite interventions in place), unexpected disease presentation/severity, vaccine breakthrough, reinfections, severely ill patients, and patients with known epidemiologic links to settings of Omicron transmission.
- WHO advises the timely reporting of genomic data to the public domain and the timely collection of metadata including clinical and epidemiologic data for careful interpretation of results.
- It is critical that all SARS-CoV-2 testing be linked to public health actions to ensure appropriate clinical care and support and to carry out contact tracing to break chains of transmission.
S gene target failure (SGTF)
- For countries with access to diagnostic tests in which at least one gene target contains the S gene target:
- Prioritize specimens with SGTF (no detection for S gene and detection for other gene targets) for sequencing confirmation of the Omicron.
- While a sudden increase in SGFT may be indicative of circulation of the Omicron since the prevalence of Alpha variant (which also causes SGTF) is very low in the vast majority of countries, confirmation of Omicron by sequencing is recommended.
- For countries without access to diagnostic tests with S gene target, enhanced surveillance and sequencing are recommended to characterize the circulating SARS-CoV-2 variants.
Retrospective sampling
- Conduct a retrospective review of available genomic sequences and S gene dropout data if available at country level, with sample collection dates dating from October 2021 through present.
- If not already done, sequence specimens with S Gene target failure in the recent past, preferably from October 2021 through present.
- Ensure timely reporting of genomic sequences to public domain (e.g., GISAID) to facilitate automated retrospective analysis;
- For countries with such capacity, wastewater sampling may be an additional tool for the retrospective and prospective investigation of Omicron in the community.
Prospective sampling
- Due to the risk of importation by incoming travelers from locations experiencing Omicron transmission, countries may increase sampling from inbound travelers. Positive rRT-PCR samples should be sequenced to confirm presence of the Omicron.
- National testing strategies should be updated to include available diagnostic tools for rapid testing
and reporting and effective decentralization of testing.
- WHO recommends that national testing capacity and genomic sequencing capabilities and appropriate planning be undertaken for possible surges in testing demand.
3.3 Vaccination
- The presence of multiple mutations of the spike protein in the receptor-binding domain suggests that Omicron may have a high likelihood of immune escape from antibody-mediated protection. However, immune escape potential from cell-mediated immunity is more difficult to predict. Overall, there are considerable uncertainties in the magnitude of immune escape potential of Omicron. Further research is needed to better understand the escape potential against vaccine- and infection- induced immunity. Research efforts are ongoing, and the data are expected to be available in the coming weeks.
- Despite uncertainties, it is reasonable to assume that currently available vaccines offer some protection against severe disease and death.
- Efforts should be intensified by public health authorities to accelerate COVID-19 vaccination coverage in all eligible populations, but with priority for populations at high risk for serious disease who remain unvaccinated or not yet fully vaccinated. These include older adults, health care workers and those with underlying conditions putting them at risk of severe disease and death.
3.4 Risk-based approach in adjusting international travel measures
- Use a risk-based approach to adjust international travel measures in a timely manner. See forthcoming WHO advice for international traffic in relation to the SARS-CoV-2 Omicron variant for additional information.
3.5 Public health and social measures (PHSM)
- The use of masks, physical distancing, ventilation of indoor space, crowd avoidance, and hand hygiene remain key to reducing transmission of SARS CoV-2, even in the context of emerging variants. However, PHSM may need to be enhanced, to further limit interpersonal contact, to control transmission with a more transmissible variant.
- The use of established PHSM in response to individual cases or clusters of cases, including contact tracing, quarantine and isolation, must continue to be adapted to the epidemiological and social context and enforced.
- Guided by risk assessment, taking into account the epidemiological situation, response capacities, vaccination coverage and public perception, as well as uncertainties related to the rapidly evolving situation of Omicron, countries should be ready to escalate PHSM in a timely manner to avoid overwhelming demands on health care services.
- For further guidance on risk-based calibration of PHSM, please see WHO guidance on Considerations for implementing a risk-based approach to international travel in the context of COVID-19.
3.6 Health care system readiness
As part of preparedness activities while studies are ongoing to better understand the phenotypic characteristics of the new VOC, and in the anticipation of possible increase in COVID-19 case-load and
associated pressure on the health system, countries are advised to ensure mitigation plans are in place to maintain essential health services, and necessary resources are in place to respond to potential surges. Tools such as the COVID-19 Essential Supplies Forecasting Tool are available for use.
3.7 Risk communication and community engagement
- Authorities should communicate information related to Omicron and potential implication for the public in a timely and transparent manner to further foster trust and increase acceptance of response measures.
- One of the most important and effective interventions in a public health response to any event is to proactively communicate with the population what is known, what is unknown and what is being done by responsible authorities to get more information and to reduce risk.
- COVID-19 information overload and misinformation should be managed at all stages of the response by providing the right information at the right time to the right people through trusted channels (e.g. community and faith leaders, family doctors and other influential members of society). There should be an information monitoring system in place to capture emerging trends to enable delivery of a targeted communication package.
- When PHSMs are adjusted, communities should be fully and regularly informed, engaged and enabled before changes are made, to allow them to take ownership of the selected PHSM. It is critical to build and foster trust, especially in contexts where there is little or no involvement of the local population in decision-making. Clear, concise and transparent risk communication, including an evidence-based rationale for adjusting measures, should be developed with communities targeted for PHSM.
- Communities will be critical to implementing population-wide PHSMs and contributing to the mitigation of the social and economic impact of certain measures (e.g. disrupting availability of food and other needed supplies).
References
- WHO Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2- variant-of-concern
- European Centre for Disease Prevention and Control. Threat Assessment Brief: Implications of the emergence and spread of the SARS-CoV-2 B.1.1. 529 variant of concern (Omicron) for the EU/EEA. https://www.ecdc.europa.eu/en/publications-data/threat-assessment-brief-emergence-sars-cov-2- variant-b.1.1.529
- Guidance for surveillance of SARS-CoV-2 variants: Interim guidance, 9 August 2021 https://www.who.int/publications/i/item/WHO_2019-nCoV_surveillance_variants
- Other references are embedded as hyper link at each section.



{kind=link}
[…] What we know about covid-19 Omicron (B.1.1.529) […]