










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



The study findings were published in the peer reviewed journal: Placenta (Science Direct).
https://www.sciencedirect.com/science/article/pii/S0143400422003083
Various studies describe the association of maternal covid-19 infection with placental morphology [9,15–19]. However, only a few studies mention the impact of placental morphological changes in COVID-19 infection on pregnancy outcomes [16,20]. Our study, by so far, is the first study that describes the placental morphological features in a large subgroup of COVID-19 infected mothers and correlates these findings with the pregnancy outcome of these mothers.
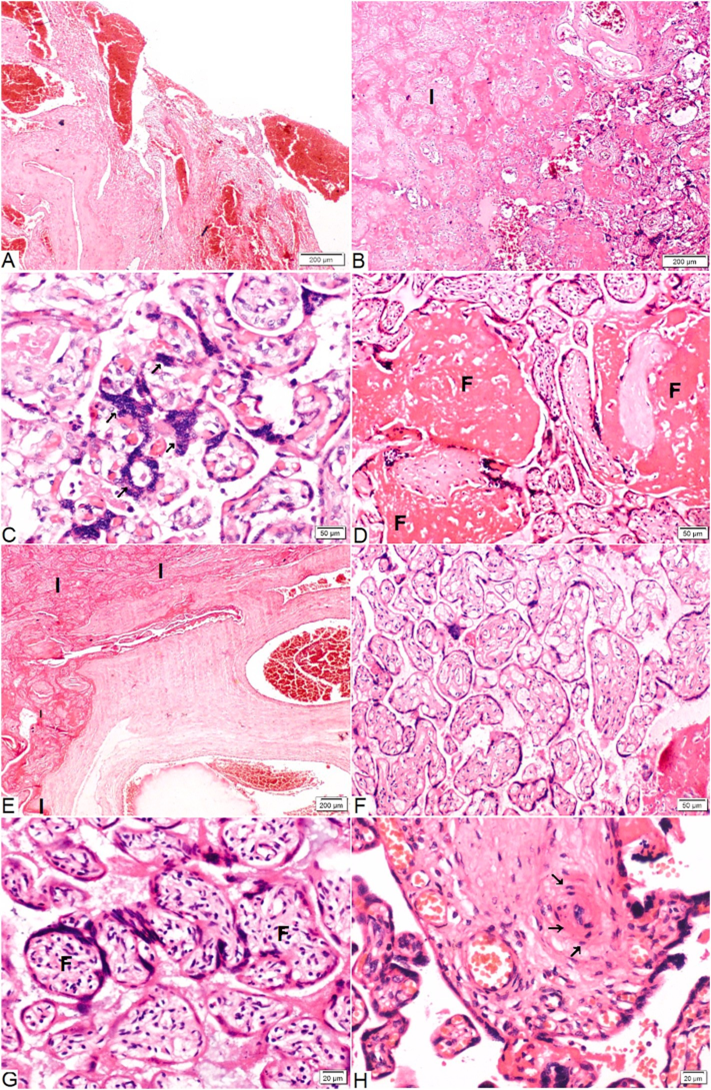
We studied 179 placentae delivered from 173 COVID-19 infected women with ≥20 weeks’ gestation. The incidence of placenta showing at least one abnormal finding on histopathological examination (HPE) in COVID-19 infected mothers was 49⋅16%. The most common abnormal finding was maternal vascular malformation (27⋅93%), followed by villous fibrin deposition (22⋅90%), fetal vasculopathy (16⋅75%), and acute inflammation (6⋅70%). The placental abnormalities were not related to the symptoms or disease severity of COVID-19 infection. Sharps et al. analysed 20 placentae and found that MVP is seen in 46% of cases, fetal vasculopathy is seen 35⋅3%, villitis in 8⋅7% cases, inter-villositis in 5⋅3% of cases, and chorioamnionitis 6% of cases [10].
Gulersen et al. also found no statistical difference in the histopathological changes in placentae delivered from COVID-19 infected women (n = 50) and matched non-COVID-19 infected women (n = 50) [9]. Hypertensive disorders of pregnancy are major risk factors for MVM [21,22].
The maternal vascular malperfusion can lead to FGR, preterm births, and stillbirths [12,23–25]. We did not find an increased incidence of pre-eclampsia or clinically detected abruptio placentae in mothers with abnormal placental pathologies (Table 3). However, we did find increased incidences of RP clots/hemorrhages on placental morphologic examination (n = 20). It can be a possibility that COVID-19 infection led to silent antepartum hemorrhages.
We also studied the outcome of neonates born to COVID-19 mothers with abnormal placental morphology and compared them with the outcomes of neonates born to COVID-19 mothers with normal placental morphology. We observed that abnormal placentae found in COVID-19 mothers led to a higher incidence of stillbirths (p-value 0⋅011). These stillbirths were clinically unexplainable as, they were not associated with higher incidence of pre-eclampsia, FGR, ICP, or abruptions.
Also, the neonates born to COVID-19 mothers with abnormal placental morphologic features had significantly lower Apgar scores at 1 min and 5 min (p-value 0⋅028 and 0⋅002, respectively). However, NICU admis-sions were not affected by the presence of abnormal placental features. Jaiswal et al. in a small comparative case-control study also studied the impact of placental injury in COVID-19 mothers (n = 27) on the preg-nancy outcome and found no significant impact on neonatal outcomes [20]. Rebutini et al. also didn’t find any significant impact of placental changes seen in COVID-19 mothers (n = 19) on their pregnancy outcome [16].
We, on the other hand, found a significant association of RP clo-t/hemorrhage and intervillous fibrin deposition with lower Apgar scores at 1 min and 5 min (Table 4). The increased systemic thrombotic events and microvascular injury syndrome seen in COVID-19 infection can affect the placenta leading to turbulent and slow blood flow, progressive rise in fibrin degradation products, decreased fibrinolysis and increased hypoxic-ischemic injury. Intriguingly, these placental changes can be so unpredictable and quiet, that early detection and intervention can be very difficult at times.
The major limitation of our study is the lack of comparison with non- COVID-19 controls. Thus, we cannot concretely say that the changes seen in our study are directly related to COVID-19 infection. The inci-dence of placental injury in COVID-19 infection in our study is nearly 50%. We agree that these changes are also seen in other pathologies and in normal cases as well and we found no effect of symptomatic/severe COVID-19 infection on the placental pathologies.
However, it can be postulated that it can affect the pregnancy outcomes leading to the higher incidence of silent abruptions, unexplained still-births, and lower Apgar scores. Therefore, vigilant antenatal and intra-partum monitoring is a must in all cases of COVID-19 infected women.
To conclude, our study is the largest descriptive-analytical research that studies the placental abnormalities in COVID-19 infection. The COVID-19 infection is associated with abnormal placental morphologic features in nearly 50% of the cases. The abnormal placental morphol-ogies seen in COVID-19 mothers are associated with poor pregnancy outcomes.
The incidence of unexplained stillbirth is significantly higher in these women. Babies born to COVID-19 mothers with abnormal placental histopathology have significantly poor neonatal Apgar scores at 1 and 5 min. Intervillous fibrin deposition and RP clots/hemorrhage are significant risk factors for lower neonatal Apgar scores at 1 min and 5 min. Villous infractions have a significant impact on the neonatal Apgar score at 5 min. Further comparative studies are required to draw a clear conclusion regarding the impact of COVID-19 infection on placenta and its effect on pregnancy outcome.



{kind=link}
[…] Up To 49 Percent Of Pregnant Women Infected With COVID-19 Will… […]
[…] Up To 49 Percent Of Pregnant Women Infected With COVID-19 Will… […]