










 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")



However, around 20% of these surgeries require a second operation, generally because cancer cells are found within the tumor margins.
Now, NIBIB-funded researchers are developing an imaging method that would allow surgeons to better identify cancerous cells in the tumor margins during surgery. This technique could lead to a reduction in follow-up breast cancer surgeries and reduce rates of breast cancer recurrence. Results were recently published in eBioMedicine.
“Today, surgeons primarily rely on their sense of sight and touch to distinguish between healthy and cancerous tissues during surgery, which may lead to incomplete removal of the tumor,” said Tatjana Atanasijevic, Ph.D., manager of the NIBIB program in Molecular Probes and Imaging Agents.
The technique relies on a method known as near-infrared imaging, which utilizes probes that fluoresce under near-infrared light. These fluorescent probes can allow clinicians to visualize features beyond the tissue surface, such as blood vessels or tumors, which can help to guide surgical procedures.
However, there aren’t many near-infrared agents that are approved for clinical use by the U.S. Food and Drug Administration (FDA), and those that are approved are non-specific, meaning that they don’t home in on a specific target in the body. Further, the only near-infrared probe approved for surgery, indocyanine green (ICG), doesn’t stay in the bloodstream for very long and therefore its utility for image-guided tumor resection is somewhat limited.
“Our research group has previously reported that p28 preferentially enters into various human breast cancer cells and actually induces anti-proliferative effects,” explained Tohru Yamada, Ph.D., an associate professor in the Department of Surgery at the University of Illinois College of Medicine and senior author of the study.
What’s more, p28 has been evaluated in early clinical trials and was well tolerated by patients. “Our new probe, termed ICG-p28, can selectively illuminate breast cancer cells under near-infrared light and thereby facilitates the image-guided removal of cancerous tissue at the time of surgery.”
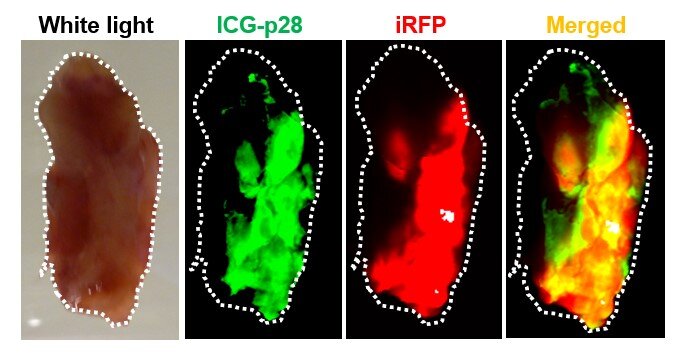
The researchers first needed to determine how well their imaging probe could accurately delineate breast cancer from healthy tissue. To do this, they created a breast cancer cell line that expresses a protein called iRFP, which fluoresces under near-infrared light. This way, when the researchers establish their breast cancer models by injecting mice with this particular cell line, they can precisely visualize the exact shape and size of the breast tumors.
After establishing the breast cancer models, the researchers then injected the mice with their imaging probe, waited 24 hours, excised the tumors, and compared the fluorescent signals between iRFP and ICG-p28. They found that the two signals had excellent overlap, indicating that their imaging probe specifically targets breast cancer tumors for an extended period of time.
Next, Yamada and colleagues used their probe to guide tumor resection in two models of breast cancer and watched the animals for cancer recurrence. Once the mice developed tumors, the researchers injected them with either ICG-p28, ICG alone, or a control buffer solution without any near-infrared dye, and waited 24 hours.
Then the tumors were removed, aided by image-guided visualization using near-infrared light, or using traditional palpation and direct visualization (for mice injected with the control buffer solution). Four weeks after the surgery, more than 30% of mice injected with the control buffer solution experienced tumor recurrence, and 25% of mice injected with ICG alone experienced recurrence.
However, just over 6% of mice injected with ICG-p28 experienced recurrence, demonstrating that the ICG-p28 probe improved surgical outcomes.
“This preclinical study demonstrated that intraoperative imaging with ICG-p28 can accurately identify tumor margins and ultimately improves the tumor recurrence rate in multiple breast cancer models,” said Yamada. “Additionally, because p28 preferentially penetrates various types of human cancer cells, we anticipate that our imaging approach can be applied to additional cancer types.”
Breast cancer is primarily treated via surgical excision of the tumour with the surrounding normal breast tissue margin. In the early stage, these treatments take the form of breast-conserving surgery (BCS) or lumpectomy.1 Although BCS provides satisfactory cosmetic outcomes, the re-resection rate is ∼20%, and of these surgeries, ∼85% are performed due to the presence of initial positive margins.2
Although there is often a need for further surgery and additional tissue removal owing to the inherent challenges in achieving negative margins, existing guidelines recommend against excising a wider negative margin in routine practice.3 Currently, surgeons rely primarily on visual and tactile cues to distinguish between healthy and malignant tissues and thus may leave residual lesions in the tumour bed.4
MRI, mammography, ultrasound, and CT etc. are readily available imaging modalities typically used to assess the tumour lesion prior to the surgical procedure. Although these traditional imaging modalities have been of immense help in advancing tumour detection and determining the extent of resection(s),5 the need for accurate intraoperative imaging remains one of the most important unmet needs in the management of breast cancer at the time of the initial BCS.
Extensive research is ongoing to identify new, rapid, and accurate intraoperative margin assessment tools, some of which are currently undergoing clinical testing.6 For example, among biophotonic-based techniques, image-guided surgery using fluorescence imaging offers many advantages for surgeons. Near-infrared (NIR) imaging is an emerging biomedical imaging modality for fluorescence-guided surgery because of its significant light absorption, ability to assist in real-time visualization, and lack of ionizing radiation.
In vivo imaging in the NIR range (700–900 nm) is superior to that in the visible spectrum owing to its low scattering, negligible tissue autofluorescence, and relatively high tissue penetration.7 The first FDA-approved NIR dye, indocyanine green (ICG), has been used in clinical practice to determine the liver function, cardiac output, and blood flow etc) for over fifty years due to its proven safety and the feasibility of its use. Also, ICG has been tested for tumour margin identification.8, 9, 10
Although ICG can localize to breast tumours, the primary disadvantages of ICG are its short half-life, and its lack of a tumour-specific interaction mechanism as a passive fluorescent dye.9,11,12 Thus, creating a new tumour-targeted version of ICG could overcome the limitations and be more useful in the clinic.
The tumour-targeted delivery of imaging agents or drugs is one of the major challenges in cancer therapy.13 As targeted delivery could improve the usefulness of such agents, various delivery vehicles, including small molecules, antibodies, proteins, and peptides, have been investigated.14
Peptides are generally more specific than small molecules due to their high complexity and are relatively inexpensive to manufacture. In particular, cell-penetrating peptides (CPPs) have been shown to be a promising agent for improving the delivery and intracellular uptake of diagnostic and therapeutic agents.15 They also have advantages over greater molecular weight antibodies in terms of feasibility of synthesis, derivatization flexibility, low immunogenicity, and physicochemical parameters.16 These characteristics suggest that the development of CPPs as carrier molecules is a promising strategy for tumour-targeted delivery.
We previously reported that Pseudomonas aeruginosa azurin and its derived peptide p28 preferentially enter various cancer cells17 and induce antiproliferative effects.18,19 As a single therapeutic agent, p28 (NSC745104) was tested in two phase I clinical trials and granted the FDA Orphan Drug and Rare Pediatric Disease designations due to its demonstrated preliminary efficacy without apparent adverse effects, toxicity or immunogenicity in patients with advanced solid tumours and in paediatric patients with recurrent and refractory central nervous system tumours (NCI and Pediatric Brain Tumor Consortium).20, 21, 22
As such, p28 is a potentially ideal CPP that can serve as a tumour-targeted carrier17,18,21,22 since it preferentially penetrates cancer cells,17,18 is highly water soluble and stable,23 and clinically exhibits no significant adverse effects, toxicity or immunogenicity in humans.21,22 Here, we developed a new noninvasive NIR-based probe, ICG-p28, composed of clinically nontoxic p28 and FDA-approved ICG. Our approach was not designed for tumour diagnosis (tumour localization).
Our experiments were specifically designed to improve the identification of positive margins, intraoperatively. We report that image-guided surgery with ICG-p28 clearly defines margins in a real-time, 3D fashion, resulting in adequate tumour excision in clinically relevant settings. These findings hold promise for improved outcomes in BCS and can guide the development of simplified (in terms of overall procedure/operation time)24 and more cost-effective protocols.
reference link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8814381/
More information: Masahide Goto et al, Image-guided surgery with a new tumour-targeting probe improves the identification of positive margins, eBioMedicine (2022). DOI: 10.1016/j.ebiom.2022.103850



{kind=link}