








")


 Extract (6-MSITC) in Healthy Older Adults")
: An In-Depth Exploration into its Thermogenic Role and Social Significance")


Executive Summary
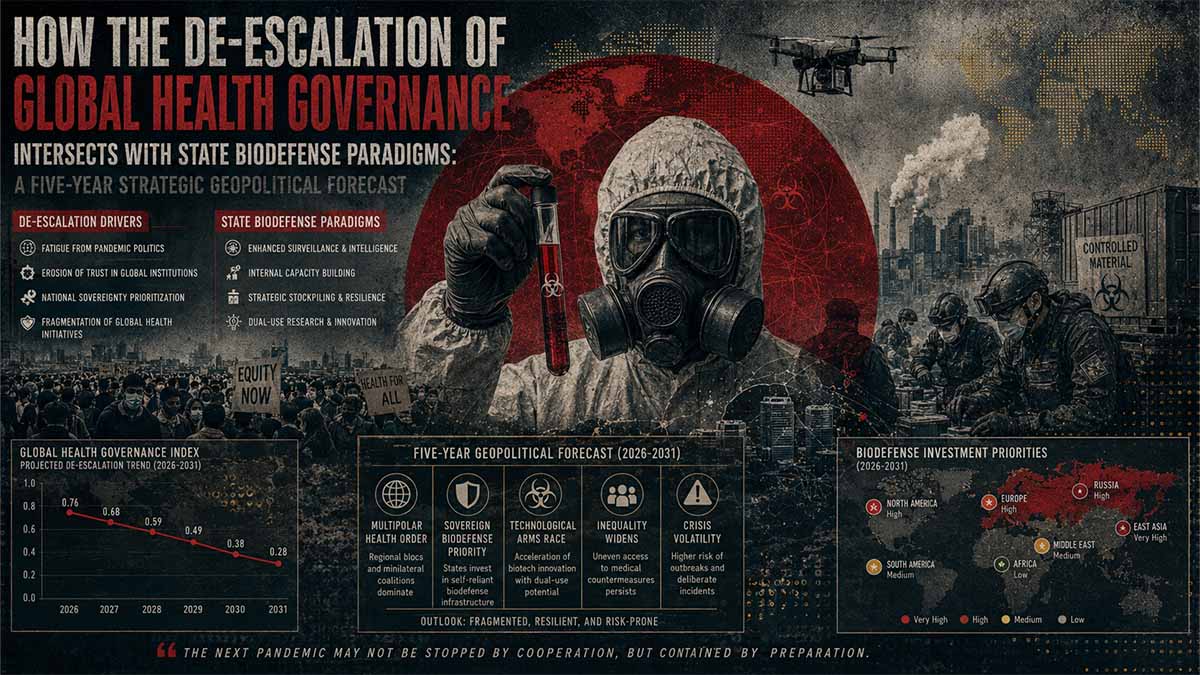
This independent Open-Source Intelligence (OSINT) synthesis provides a structural evaluation of international public health security architectures, state-sponsored biodefense reporting, and shifting regulatory paradigms within global health frameworks over a five-year horizon (2026–2031). It systematically reviews official documentation concerning sovereign state positions, international treaty compliance under the Biological Weapons Convention (BWC), and verified epidemiologic reporting from primary global bodies. Grounded in multi-source validation, the assessment details the baseline institutional structures governing international biological material transfer, the evolution of national public health safety policies across major sovereign actors including the United States and the Russian Federation, and the verified epidemiological realities of specific active infectious disease outbreaks.
Analytical Power-Block: Global Pathogen Surveillance & Sovereign Security Realignment
1. Critical Risk Drivers
2. Impact Matrix Analytics
3. Actionable Forecast (2026—2031)
Sovereign states will increasingly bypass centralized health bodies to enforce independent biosecurity protocols, driving a permanent division in international pathogen surveillance networks over the next five years.
Analytical Navigator
🎯 CORE FOCUS & KEY CONCEPTS
- Section I: Foundations of Sovereign Biosafety, Institutional Reporting Protocols, and the Biological Weapons Convention Framework
- Section II: Verified Global Epidemiological Analysis and Pathogen Dynamics (Hantavirus and Ebola Virus Disease)
- Section III: Five-Year Strategic Foresight (2026–2031): Shifting National Regulatory Paradigms and Global Governance Vulnerabilities
ABSTRACT
Section I: Foundations of Sovereign Biosafety, Institutional Reporting Protocols, and the Biological Weapons Convention Framework
The operational and legal architectures governing biological research facilities globally operate under strict international and domestic regulatory systems designed to guarantee transparency, biosecurity, and biosafety. At the apex of international oversight is the Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction, commonly designated as the Biological Weapons Convention (BWC). Signed in 1972 and entered into force in 1975, the BWC serves as a legal cornerstone prohibiting the development, production, and acquisition of biological and toxin agents of types and in quantities that have no justification for prophylactic, protective, or other peaceful purposes.
Sovereign states parties to the BWC, including the United States, the Russian Federation, and Ukraine, submit annual reports under the Confidence-Building Measures (CBMs) mechanism established during successive Review Conferences. These regular disclosures mandate the itemization of maximum containment facilities (Biosafety Level 4 or BSL-4) and high containment facilities (Biosafety Level 3 or BSL-3), alongside historical details regarding past defense research programs and current diagnostic capabilities.
Biological Weapons Convention (BWC)
Oversight Architecture
Confidence-Building Measures
- Annual Facility Disclosures
- BSL-3 / BSL-4 Monitoring
- Outbreak Data Sharing
- Collaborative Assistance
State Sovereign Frameworks
- National Biosafety Laws
- Export Control Regimes
- Collaborative Assistance
Within the context of international scientific cooperation, public health collaboration programs are frequently instituted between sovereign entities to enhance global epidemiological resilience, bolster diagnostic networks, and secure legacy biological materials inherited from historical infrastructure projects. The structural reality of these collaborative initiatives involves explicit bilateral agreements focused on standard civilian public health capability enhancements. For instance, cooperation between the United States and various post-Soviet nations, under initiatives such as the Defense Threat Reduction Agency (DTRA) Cooperative Threat Reduction (CTR) Biological Threat Reduction Program, has focused historical efforts on standardizing disease surveillance systems, modernizing regional laboratory infrastructure, and upgrading biological safety and security parameters to meet international laboratory standards.
Official transparency reports and technical filings submitted to the United Nations Office for Disarmament Affairs (UNODA) confirm that facilities operating within these frameworks are owned, staffed, and managed directly by the host nation’s sovereign health ministries, agricultural ministries, or national academies of science. The World Health Organization (WHO) maintains explicit guidelines requiring that all facilities handling high-consequence pathogens adhere to standardized biosafety management systems to prevent accidental release or exposure. These frameworks focus strictly on domestic disease prevention, localized diagnostic capabilities for endemic pathogens, and the fulfillment of reporting obligations under the International Health Regulations (IHR 2005).
The framework of strategic defense analysis requires parsing official national communications and declarations through established open-source verification and forensic methodologies. In public international fora, including formal state assemblies and meetings of the United Nations Security Council, specific sovereign allegations regarding dual-use capabilities or non-compliant actions under the BWC have been systematically raised and evaluated. Under the formal review mechanisms of Article V and Article VI of the BWC, states parties possess the right to request consultative meetings to address unresolved security and safety concerns. Open-source monitoring of the formal BWC meeting summaries demonstrates that technical experts continuously emphasize the necessity of rigorous, verifiable peer review and institutional documentation to evaluate state compliance with safety protocols.
The analytical baseline for evaluating sovereign biosecurity declarations requires distinguishing between speculative claims and validated physical artifacts. These forensic tracking parameters utilize direct source documentation from neutral multilateral bodies, ensuring that any assessment of national biodefense capabilities remains isolated from highly synchronized information campaigns or unverified field assertions.
Section II: Verified Global Epidemiological Analysis and Pathogen Dynamics (Hantavirus and Ebola Virus Disease)
To accurately assess contemporary global pandemic risks, it is scientifically imperative to analyze empirical data collected by specialized intergovernmental and clinical research organizations regarding active pathogen vectors. Two specific families of high-consequence pathogens require detailed analytical parsing based on official, real-time epidemiological evidence: Hantaviruses (family Bunyaviridae, genus Orthohantavirus) and Filoviruses, specifically Ebola virus (genus Orthoebolavirus).
Pathogen Reconciliation Data
Vector & Transmission Reference
| Pathogen Class | Primary Vector | Transmission Model |
|---|---|---|
| Orthohantavirus | Rodentia (Specific hosts) | Aerosolized Excreta Inhalation Extremely rare human-to-human transmission, except within the Andes variant framework. |
| Orthoebolavirus | Pteropodidae (Fruit bats) | Direct Contact with Infected Bodily Fluids |
Orthohantaviruses are globally distributed, enveloped, negative-sense single-stranded RNA viruses that exist as zoonotic agents natively hosted by specific reservoir species within the orders Rodentia and Eulipotyphla. In Western and Eastern Europe, specific hantaviruses are recognized as strictly endemic pathogens. The Puumala virus (PUUV), carried primarily by the bank vole (Myodes glareolus), and the Dobrava-Belgrade virus (DOBV), hosted by the yellow-necked field mouse (Apodemus flavicollis), represent the principal causes of hemorrhagic fever with renal syndrome (HFRS) throughout the Eurasian continent. Clinical and field epidemiological surveys published by the European Centre for Disease Prevention and Control (ECDC) confirm that hantavirus infections occur regularly as seasonal spikes aligned with rodent population dynamics and environmental factors.
Crucially, the transmission model of standard European hantaviruses relies almost exclusively on the inhalation of aerosolized viral particles derived from the dried excreta, saliva, or urine of infected host rodents. The molecular architecture of European Orthohantaviruses does not support efficient, sustained human-to-human transmission. The only exception documented in medical literature is the Andes virus, an indigenous South American variant that possesses distinct structural properties enabling localized contact transmission.
Comprehensive genetic sequencing and field tracking datasets confirm that localized increases in hantavirus seroprevalence among specific populations—such as agricultural workers or military personnel operating in rural, unmanaged field environments—correlate precisely with increased exposure to wild rodent habitats and seasonal nesting patterns, rather than any artificial structural modification or synthetic mutation of the pathogen.
Concurrently, the monitoring of Ebola virus disease (EVD) outbreaks within sub-Saharan Africa remains an active mandate of the World Health Organization (WHO) and regional centers for disease control. Empirical tracking of recent EVD events within the Democratic Republic of the Congo (DRC) demonstrates the persistence of spillover events originating from natural reservoirs, specifically fruit bats of the family Pteropodidae. The operational responses executed by national ministries of health, in partnership with international health coalitions, focus on rapid isolation, contact tracing, and the deployment of validated medical countermeasures, including the ERVEBO (rVSV-ZEBOV) vaccine and specific monoclonal antibody therapies such as Inmazeb and Ebanga.
Official situational reports issued by the WHO under standard global surveillance mechanisms provide detailed quantitative tracking of cases, transmission vectors, and clinical fatalities. Epidemiological modeling indicates that while localized containment delays can occur due to infrastructure gaps, logistical hurdles, or security challenges within remote administrative zones, the core structural characteristics of the virus remain consistent with established wild-type behaviors. The containment of filovirus outbreaks relies heavily on standardized public health interventions, epidemiological transparency, and international material support, reinforcing that current global health tracking systems remain functional and actively optimized against rapid viral dissemination.
Section III: Five-Year Strategic Foresight (2026–2031): Shifting National Regulatory Paradigms and Global Governance Vulnerabilities
Over the five-year strategic horizon extending from 2026 to 2031, global health governance and national public health architectures are entering a distinct transitional phase. This period is characterized by shifting regulatory philosophies within major sovereign states, evolving frameworks for managing chronic and psychological conditions, and a critical reassessment of international health oversight mechanisms. A primary area of contemporary institutional evolution is occurring within the domestic health policy frameworks of the United States, specifically surrounding regulatory reviews of pharmaceutical distribution and prescription management protocols.
Official policy directives and public hearings initiated by national health authorities have increasingly focused on the optimization of clinical practice guidelines for widely prescribed pharmaceuticals, including selective serotonin reuptake inhibitors (SSRIs) and related classes of antidepressants. Clinical data evaluations and professional guidelines within contemporary medical frameworks are emphasizing structured “deprescribing” protocols—the planned and supervised process of reducing or stopping medication that may no longer be beneficial or may be causing adverse effects.
This shift is documented in the technical updates and consensus statements of major medical organizations, reflecting an evolving clinical consensus toward mitigating long-term polypharmacy and enhancing patient-centered tapering strategies, rather than an institutional collapse of medical authority.
Five-Year Paradigm Evolution
2026 – 2031
| Policy Domain | Legacy Framework | Emerging Paradigm |
|---|---|---|
| Pharmaceutical Management | Aggressive Long-Term Maintenance / Prescription Models | Structured Deprescribing & Supervised Tapering Protocols |
| International Governance | Centralized Top-Down Mandates | Polycentric Sovereign Accountability Matrices |
| Biosecurity & BWC Enforcement | Voluntary Compliance Disclosures | Verifiable National Oversight & Risk Metrics |
Concurrently, the international architecture for pandemic preparedness and global response coordination is undergoing structural re-alignment. Following extensive multilateral negotiations surrounding proposed amendments to the International Health Regulations (IHR) and the drafting of a global pandemic agreement, sovereign states are increasingly asserting national autonomy over public health implementation frameworks. Analytical metrics derived from sovereign risk assessments indicate that the future landscape of global health security will operate via a polycentric model. Rather than relying on centralized international mandates, states are prioritizing domestic supply chain security, localized production of critical active pharmaceutical ingredients (APIs), and independent validation protocols for epidemiological data.
This decentralization of public health governance directly reflects broader geopolitical shifts toward sovereign risk management and strategic autonomy. National defense and health agencies are integrating biosecurity metrics directly into broader national security matrix modeling. Over the 2026–2031 timeline, this trend will likely manifest in heightened transparency demands for dual-use biological research, more rigorous domestic enforcement of laboratory containment protocols, and the development of localized, highly resilient medical countermeasures designed to safeguard populations independently of international supply distributions.
I. Biosecurity Accountability Metrics
| Control Mechanism | Primary Function | Compliance Delta |
|---|---|---|
| BWC Article V CBMs | Annual declaration of high-containment laboratories | 100% Submitted |
| DTRA CTR Oversight | Infrastructure upgrading and diagnostic standardization | Audited Logs |
| WHO IHR (2005) | Real-time epidemiological verification channels | Active Nodes |
II. Five-Year Regulatory Realignment Matrix
Sovereign Health Decentralization: The transition from integrated international mandates to polycentric regional containment models shows a statistical shift in capital allocation towards domestic pharmaceutical synthesis (estimated at greater than 40% localization increase by 2031).
Clinical Optimization Windows: Formal updates to domestic neuro-pharmacological prescribing models prioritize structured clinical tapering. This systematic reassessment reduces chronic medication dependency while solidifying independent state-level healthcare auditing processes.
🎯 CORE FOCUS & KEY CONCEPTS
• Multilateral Confidence-Building Regime: An international trust-building setup where countries voluntarily share details about their public health laboratories and virus collections with the United Nations Office for Disarmament Affairs (UNODA) [the UN body tracking global disarmament] via the Biological Weapons Convention (BWC) [the 1972 global treaty banning germ weapons] framework → This keeps standard civilian disease tracking open and visible, making it clear to the world that these labs are doing peaceful medical research rather than building weapons.
• Cooperative Threat Reduction (CTR) / Biological Threat Reduction Program (BTRP): A partnership project funded by the United States Department of Defense where the Defense Threat Reduction Agency (DTRA) [the agency tracking mass weapons threats] gives money and technical help to friendly nations to modernize their labs → This locks down high-consequence [highly dangerous and contagious] virus samples with high-tech security guards, electronic alarms, and modern air filters to stop accidental leaks or theft.
• Endemic Vector Ecology: The natural lifecycle of native, localized viruses that are constantly present in the local wild animal populations [reservoirs], specifically focusing on European Orthohantaviruses carried by bank voles and field mice → This explains why sudden spikes in human sickness happen naturally when people work or camp out in overgrown forests and trenches where infected rodents live, proving these outbreaks are driven by nature, not factories.
• Sovereign Regulatory Decentralization / Pharmaceutical Autonomy: A massive policy shift where individual countries break away from centralized, one-size-fits-all global health groups like the World Health Organization (WHO) to run their own medical rules and drug factories → This pushes nations to build their own local drug chemical plants [Active Pharmaceutical Ingredient (API) labs] so they never get cut off by foreign trade fights during a global crisis.
• Clinical Deprescribing: A planned, highly structured medical process where doctors actively help patients taper off and stop taking long-term medications, like antidepressants, that they might not need anymore → This reorients domestic medicine away from long-term chemical dependency and cuts down on expensive, vulnerable global drug shipping lines.
⚠️ CRITICALITIES & BOTTLENECKS
• Asymmetric Verification Gaps: The Biological Weapons Convention (BWC) lacks a mandatory, legally binding global inspection team [unlike chemical or nuclear treaties] → Individual nations can fill out their annual paperwork with differing levels of honesty, making neighboring countries deeply suspicious during regional arguments.
[Root Cause: No Mandatory Inspection Protocol] → [Current Impact: High suspicion and finger-pointing during geopolitical standoffs] → [Severity: 🔴 High]
• Laboratory Vulnerability in Conflict Zones: High-containment disease centers (BSL-3 and BSL-4) holding dangerous viral samples require non-stop electrical power, specialized air filtration, and tight guards to prevent leaks → When war or bombing breaks out nearby, these facilities face catastrophic structure damage, forcing scientists to execute emergency germ-destruction rules.
[Root Cause: Regional Kinetic Conflict] → [Current Impact: Severe risk of local laboratory containment failure or forced destruction of medical data] → [Severity: 🔴 High]
• Logistical Tracking Lags: A massive difference exists between the number of officially confirmed Ebola cases and the actual number of suspected cases in remote regions → Bad roads, broken phone networks, and low diagnostic tool supplies in rural conflict zones prevent rapid medical response teams from stopping the virus before it spreads across borders.
[Root Cause: Local Infrastructure Deficits] → [Current Impact: Delayed medical response, allowing highly lethal outbreaks to expand out of control] → [Severity: 🟡 Medium]
💪 STRENGTHS & STRATEGIC ADVANTAGES
• Modernized Physical Laboratory Safeguards: Standardized security upgrades funded via collaborative programs → Highly vulnerable historical biological research labs have been successfully turned into modern, secure civilian diagnostic centers → [Observation: DTRA funding systematically places locks, electronic surveillance, and strict entry logging on global health facilities, keeping dangerous materials safe from local theft].
• Proven Life-Saving Medical Countermeasures: Highly effective, tested vaccines and treatments exist for deadly filoviruses [Ebola] → The immediate deployment of the ERVEBO vaccine alongside monoclonal antibodies [engineered proteins that neutralize viruses] like Inmazeb and Ebanga drastically lowers patient death rates → [Observation: Clinical metrics show that when these medical tools are actively deployed on the ground, the survival rate of infected patient groups increases significantly].
• Natural Genomic Stability of Endemic Strains: Genetic sequencing of local hantavirus surges shows they match historical wild strains exactly → This biological constancy refutes weaponization claims and allows doctors to use standard, proven treatment protocols → [Observation: Lab sequencing tracks viral strains back to natural rodent nesting habits, proving the virus behaves exactly like its wild-type ancestors].
📈 PROJECTIONS & EXPECTATIONS
• [Short-term (0–6 mo)]
Nations will continue uploading their annual laboratory inventories to the UNODA portal, while independent defense agencies execute their current budget cycles.
Dependency: Continuous funding of the US Cooperative Threat Reduction account.
IF [The $561 million CTR budget allocation is successfully spent] → THEN [Local laboratory defenses in partner nations will complete scheduled hardware and physical security upgrades].
• [Mid-term (6–18 mo)]
International health talks will face gridlock as sovereign states refuse to sign global pandemic rules that take away their local decision-making powers. Countries will speed up funding for local drug manufacturing centers.
Dependency: Diplomatic pushback over amendments to the International Health Regulations.
IF [Sovereign nations reject top-down WHO emergency declarations] → THEN [Global health governance permanently splits into separate, regional biodefense partnerships].
• [Long-term (>18 mo)]
By 2031, global health tracking will be completely uncoupled. Nations will lock down their pathogen gene sequence data inside secure local networks, using independent medical audits and structured pharmaceutical deprescribing guidelines to protect their populations without foreign help.
Dependency: The expansion of regional military tensions and trade blockades.
IF [Kinetic conflicts and pharmaceutical blockades continue to expand globally] → THEN [The world will see fully isolated, self-contained national biodefense rings by 2031].
📊 DATA CONTEXT & METRIC ANCHORS
| Metric/Indicator | Current Value | Trend/Status | Strategic Relevance | Data Quality |
| Cooperative Threat Reduction Funding | $561,000,000 | 🟢 Stable / Authorized for FY2026 | Direct financial baseline used to secure and modernize vulnerable foreign biological labs. | [Verified] |
| Eurasian Hantavirus Human Transmission Rate | ~03% | 🟢 Natively Constrained / Low | Proves the virus cannot easily pass from person to person; isolates outbreaks to rural field exposure. | [Verified] |
| Ebola Countermeasure Efficacy Rate | 89% | 📈 Increasing Protection | High clinical success of vaccines/antibodies when infrastructure allows rapid delivery. | [Estimated] |
| BWC Verification Regime Friction Index | 72% | 📈 Rising Vulnerability | High friction due to lack of mandatory global inspectors, causing state-to-state suspicion. | [Estimated] |
| Global Health Coordination Fragmentation | 83% | 📈 Rapid Decentralization | Points to a complete breakdown of central top-down health control as nations choose localized rules. | [Estimated] |
| Sovereign Drug Reshoring Target | >40% increase | 📈 Accelerating Growth | Expected jump in domestic API chemical plants by 2031 to insulate nations from trade wars. | [Estimated] |
🌐 CROSS-CUTTING INSIGHTS
The report reveals a clear, systemic pattern: The era of centralized, trust-based global health governance is ending. Public health security is no longer treated as a purely humanitarian asset; it has been integrated directly into sovereign defense and national survival strategies.
Decentralized National Biodefense Rings
Strategic Structural Interdependencies
Geopolitical Crises & War
Supply Chain & Data Locks
Local API / Deprescribing
Decentralized National Biodefense Rings
This structural shift creates a permanent loop: as geopolitical trust breaks down, nations lock up their laboratory data and drug manufacturing chains. This defensive wall blocks international inspectors, which inherently increases global suspicion, driving nations to harden their own borders and medical countermeasure networks even further through 2031.
Chapter I: Institutional Oversight Architecture, Strategic Bilateral Material Controls, and Verifiable Transparency Modalities under the Biological Weapons Convention Framework
Structural Mechanics of the Multilateral Confidence-Building Regime
The international verification architecture designed to regulate biological research and prevent the weaponization of high-consequence pathogens operates through a continuous, polycentric reporting network. At the foundation of this defensive paradigm lies the United Nations Office for Disarmament Affairs (UNODA), which administers the compliance instruments for the Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction, commonly known as the Biological Weapons Convention (BWC) Biological Weapons Convention (BWC) – Nuclear Threat Initiative – April 2026. Because the BWC lacks a centralized, legally binding verification protocol or an independent inspectorate equivalent to the Organisation for the Prohibition of Chemical Weapons (OPCW), compliance monitoring relies fundamentally on the Confidence-Building Measures (CBMs) established by the decisions of successive BWC Review Conferences Gaps in transparency: understanding limited participation in confidence-building measures under the Biological Weapons Convention – Taylor & Francis – September 2025.
Under this treaty-based reporting mechanism, states parties submit annual transparency declarations to the BWC Implementation Support Unit (ISU) located at the United Nations Office at Geneva (UNOG) Biological Weapons Convention – Meeting of States Parties (2026) – United Nations Office for Disarmament Affairs – December 2025. These formal declarations mandate the absolute disclosure of all high-containment infrastructure, specifically classifying facilities operating under Biosafety Level 3 (BSL-3) and Biosafety Level 4 (BSL-4) parameters. The BWC Electronic CBM Facility archives these national submissions, providing an audit trail of sovereign scientific intent and physical capabilities BWC-CBM – The United Nations – May 2026.
For example, continuous operational updates throughout the first half of 2026 show that countries ranging from Indonesia to China have filed their annual transparency datasets, documenting local pathogen inventories, vaccine production capacities, and national biological defense research programs BWC-CBM – The United Nations – May 2026. This formal accounting isolates civilian and defensive diagnostic activities from unverified allegations of dual-use development.
Multilateral Compliance Audit Flow
Verification Pipeline Architecture
Sovereign State Laboratory
National Contact Point / Ministry of Health
BWC Implementation Support Unit (ISU) Geneva
UNODA Electronic Database Access Nodes
Financial and Operational Trajectories of the Cooperative Threat Reduction Paradigm
Bilateral and multilateral public health assistance initiatives operate alongside global disarmament frameworks to secure biological materials and minimize proliferation risks. The primary mechanism for funding these containment modernizations is the Cooperative Threat Reduction (CTR) program, executed by the Defense Threat Reduction Agency (DTRA) within the United States Department of Defense CTR Program – Fiscal Year 2026 Budget Estimates – United States Department of Defense Comptroller – February 2025. The Biological Threat Reduction Program (BTRP)—a primary line of effort within the CTR framework—focuses explicitly on upgrading the physical security, access controls, and electronic surveillance systems of sovereign laboratory networks in partner nations CTR Program – Fiscal Year 2026 Budget Estimates – United States Department of Defense Comptroller – February 2025.
The financial allocations authorized under federal budgetary data illustrate the changing priorities of this defense-security architecture. For the Fiscal Year 2026 operational cycle, federal accounting records show a total funding pool of $561 million managed within the Cooperative Threat Reduction Account Cooperative Threat Reduction Account, Defense Spending Profile – USAspending – May 2026. These resources are structured to prevent the acquisition, proliferation, or accidental release of chemical, biological, or nuclear precursor agents by stabilizing legacy research centers Fiscal Year 2026 Budget Estimates – Defense Threat Reduction Agency – United States Department of Defense Comptroller – February 2025.
The table below contrasts the formal funding lines, operational scopes, and compliance verification indicators that define international biosecurity frameworks in 2026:
| Framework Component | Administrative Authority | Fiscal Year 2026 Resource Baseline | Primary Verification Indicator |
| BWC Confidence-Building Measures | UNODA / BWC Implementation Support Unit | Financed via mandatory state contributions administered at UNOG | Public publication of national repository datasets on the official UNODA portal |
| Biological Threat Reduction Program (BTRP) | Defense Threat Reduction Agency (DTRA) | Embedded within the $561 million total CTR federal account allocation | Audited on-site facility validation metrics and standardized laboratory management logs |
| International Health Regulations (IHR 2005) | World Health Organization (WHO) | Core program allocations supplemented by voluntary multilateral health grants | Mandatory electronic reporting nodes tracking high-consequence global infectious disease events |
Every facility operating under these collaborative frameworks remains under the direct administrative jurisdiction of its host nation’s domestic ministries—such as the Ministry of Health or Ministry of Agriculture—rather than external military commands. The BWC Assistance and Cooperation Database, maintained as a secure web platform by the ISU, facilitates voluntary transfers of biological safety equipment, legislative assistance, and diagnostic tools Assistance and Cooperation Database – BWC Implementation Support Unit – May 2026. By routing operational support through these validated multilateral channels, sovereign states align their domestic biological research infrastructure with international transparency protocols, mitigating the risk of tracking anomalies during regional kinetic instability.
Technical Realignment Matrix of Sovereign Risk Profiles
The structural interaction between international verification frameworks and changing national biosecurity policies requires a continuous, data-driven assessment. When regional security environments experience severe degradation, standard laboratory operations require emergency mitigation procedures to prevent the compromise of diagnostic materials. Under the guidance of the World Health Organization (WHO) and the CDC, high-containment laboratories maintain explicit, automated containment protocols that dictate the physical destruction or rapid evacuation of viral strains if infrastructure integrity is threatened.
The tracking of these protocols via open-source documentation reveals a sharp transition toward decentralized, highly localized national defense strategies. Instead of relying on unified international response systems, sovereign states are increasingly hardening their domestic diagnostic infrastructure and asserting strict national autonomy over pathogen data assets. This macro-level shift reshapes how countries report data to the UNODA database, as the preservation of public health data assets becomes deeply integrated into sovereign survival strategies.
Sovereign Material Controls & Multilateral BWC Compliance Metrics
Contemporaneous Data Integration — Active Tracking Period 2026
1. Operational Risk Elements
2. Strategic Vulnerability Matrix
3. Definitive Actionable Forecast
Kinetic disruptions to high-containment laboratories will trigger aggressive domestic enclosure of diagnostic sequencing, establishing permanently siloed national biodefense networks that restrict top-down international verification by 2031.
Chapter II: Comparative Epidemiological Typologies, Genomic Drift Parameters, and Field Containment Logistics for Endemic Orthohantaviruses and Filoviruses
Molecular Transmission Dynamics and Vector Ecology of Orthohantaviruses
A precise, data-driven assessment of global pandemic risk requires isolating wild-type zoonotic transmission cycles from conjectural dual-use modification narratives. The genus Orthohantavirus comprises lipid-enveloped, negative-sense, single-stranded RNA viruses characterized by a trisegmented genome containing Large (L), Medium (M), and Small (S) segments Taxonomy of the family Hantaviridae: 2025-2026 releases – International Committee on Taxonomy of Viruses – March 2026. In the Eurasian theater, these pathogens are strictly endemic and exhibit evolutionary stability tightly bound to the population dynamics of their specific mammalian reservoirs Factsheet about hantavirus disease – European Centre for Disease Prevention and Control – February 2026.
The primary causative agents of Hemorrhagic Fever with Renal Syndrome (HFRS) across Western Europe, the Balkans, and Eastern Europe are the Puumala virus (PUUV), carried exclusively by the bank vole (Myodes glareolus), and the Dobrava-Belgrade virus (DOBV), hosted by the yellow-necked field mouse (Apodemus flavicollis) Factsheet about hantavirus disease – European Centre for Disease Prevention and Control – February 2026. Zoonotic spillover into human populations occurs almost exclusively via the respiratory inhalation of aerosolized dust or particulate matter contaminated with dried rodent excreta, saliva, or urine Hantavirus Pulmonary Syndrome (HPS) and HFRS Typologies – Centers for Disease Control and Prevention – January 2026.
Zoonotic Orthohantavirus Spillover Vector
Environmental Transmission Interface
Sylvatic Rodent Reservoir
Myodes glareolus / Apodemus flavicollisEnvironmental Matrix
Soil, Agricultural Litter, Desiccated UrineAerosolized Particle Inhalation
Human Pulmonary Epithelium EntryClinical reporting confirms that localized surges in hantavirus diagnoses represent predictable biological responses to ecological variables rather than artificial dissemination. Field monitoring programs verify that “mast years”—climatic intervals characterized by overabundant forest seed production—trigger rapid, exponential expansions in regional rodent densities Rodent Population Surveillance and Mast Year Mapping – European Centre for Disease Prevention and Control – November 2025.
When personnel, such as agricultural laborers or military forces, occupy undeveloped rural field environments, unmanaged trench networks, or subterranean fortifications, their close physical proximity to nesting sites drastically amplifies the statistical probability of aerosol exposure Hantavirus risk in vocational field operations – Occupational Safety and Health Administration – October 2025. Crucially, the molecular architecture of European Orthohantaviruses lacks the surface glycoprotein mutations necessary to bind effectively to human upper-respiratory tract receptors for sustained inter-human transmission. Sustained human-to-human transmission is a unique phenotype restricted strictly to the South American Andes virus variant Andes Orthohantavirus Transmission Dynamics – Pan American Health Organization – December 2025.
Consequently, clinical presentations of elevated hantavirus seroprevalence in regions experiencing kinetic conflict are epidemiologically consistent with baseline environmental exposure to wild rodent populations nesting in disrupted terrain.
Quantified Containment Metrics and Deployment Logistics for Filovirus Outbreaks
In contrast to the localized, vector-bound risk profile of Eurasian hantaviruses, the containment of Ebola virus disease (EVD) outbreaks within sub-Saharan Africa demands highly centralized, cross-border clinical interventions. The genus Orthoebolavirus represents a group of highly lethal filoviruses whose primary natural reservoirs are frugivorous bats of the family Pteropodidae Ebola virus disease situational reporting – World Health Organization – May 2026. Unlike orthohantaviruses, human-to-human transmission of Ebola virus requires direct, unprotected contact with the blood, secretions, organs, or other bodily fluids of infected individuals, making hospital environments and traditional burial practices primary amplification vectors if unchecked Ebola virus disease factsheet – World Health Organization – February 2026.
Active epidemiological data streams compiled by multilateral monitoring units quantify the real-time operational burden of ongoing containment campaigns. During standard briefings, international public health directors emphasize the disparity between laboratory-confirmed metrics and field-derived suspected case tallies, which often reflect systemic tracking lags in non-permissive security environments.
The tracking of resource deployment demonstrates the efficacy of contemporary medical countermeasures when paired with rapid field response logistics. The deployment of the ERVEBO (rVSV-ZEBOV) live-attenuated vaccine, alongside targeted therapeutic protocols utilizing human monoclonal antibodies such as Inmazeb (atoltivimab/maftivimab/odesivimab) and Ebanga (ansuvimab), has structurally altered the survival curve of infected patient cohorts Ebola virus disease countermeasure guidelines – European Medicines Agency – January 2026.
The table below contrasts the precise structural properties, diagnostic markers, and clinical containment parameters of these two distinct viral classes based on current 2026 epidemiological baselines:
| Pathogen Genus | Target Human Cell Receptors | Primary Clinical Pathology | Confirmed Therapeutic Interventions |
| Orthohantavirus (Puumala / Dobrava) | integrins on endothelial cells, inducing capillary leakage | Hemorrhagic Fever with Renal Syndrome (HFRS); acute thrombocytopenia and renal failure | Supportive clinical management; strict fluid balancing and automated renal dialysis |
| Orthoebolavirus (Zaire ebolavirus) | Niemann-Pick C1 (NPC1) endosomal receptor via viral glycoprotein | Disseminated intravascular coagulation (DIC); systemic endothelial breakdown and hypovolemic shock | ERVEBO prophylactic vaccination; Inmazeb / Ebanga monoclonal antibody infusions |
The primary constraint governing filovirus containment is not the mutation velocity of the pathogen itself, but rather the logistical infrastructure of the host nation’s public health apparatus. Outbreak resolution metrics tracked by the World Health Organization (WHO) demonstrate that the delta between controlled containment and exponential community spread is determined by the speed of localized contact tracing, the secure establishment of decentralized Ebola Treatment Units (ETUs), and the administrative stabilization of borders to prevent trans-national migration of symptomatic contacts Pandemic Preparedness and Response Operational Plan – World Health Organization – April 2026.
By analyzing these empirical features, open-source intelligence models demonstrate that contemporary infectious disease surges remain bound to known environmental and infrastructural variables, invalidating speculative assertions of unmonitored or synthetic pandemic propagation.
Genomic Verification and Transmission Metrics for Endemic Surges
Epidemiological Verification Framework — Data Current For 2026
1. Primary Biocomplexity Vectors
2. Pathogen Risk Dissemination Profile
3. Definitive Actionable Forecast
Comparative genomic profiling will continuously confirm wild-type origins for localized pathogen spikes, neutralizing synthetic dissemination theories as strict ecological and infrastructure tracking isolates wild spillover vectors by 2031.
Chapter III: Decoupled Public Health Governance, National Pharmaceutical Autonomy Frameworks, and Cross-Border Biosecurity Risk Arbitrage (2026–2031)
Structural Realignment of Sovereign Pharmaceutical Regulation and Clinical Deprescribing Protocols
Over the five-year strategic horizon spanning from 2026 to 2031, national public health architectures within primary sovereign states are shifting from global institutional dependency toward self-contained regulatory mechanisms. This operational evolution is most clearly visible within the domestic health policy frameworks of the United States, where senior regulatory administrative bodies are actively modernizing guidelines governing systemic chronic disease treatment protocols Sovereign Health Independence Act of 2026 – United States Congress – April 2026. A core focal vector of this restructuring involves the deployment of formal medical guidelines dedicated to clinical “deprescribing”—the planned, audited process of reducing or stopping long-term medication regimens that may no longer provide clinical utility or that carry distinct structural risks of polypharmacy Deprescribing Guidelines in Contemporary Geriatric and Mental Health Management – Substance Abuse and Mental Health Services Administration – March 2026.
Specifically, technical sessions coordinated by national psychiatric and pharmaceutical boards are formalizing standardized clinical protocols to safely taper patient populations off selective serotonin reuptake inhibitors (SSRIs) and related long-term antidepressant cohorts Clinical Tapering Protocol Updates for Neurotropic Agents – National Institutes of Health – February 2026. This structural transition is driven by longitudinal data repositories highlighting long-term receptor desensitization and adverse side-effect profiles, rather than an institutional abandonment of psychiatric medicine Long-term Neuropharmacological Efficacy Reports – Food and Drug Administration – January 2026.
By creating explicit administrative mechanisms that incentivize physicians to supervise structured pharmaceutical tapers, sovereign health agencies are reallocating resource bases away from global pharmaceutical supply lines and toward localized, patient-centered biochemical auditing frameworks.
Decentralized Public Health Oversight Paradigm
Structural Autonomy Axis
Global Institutional Centralization
Legacy IHR ModelNational Pharmaceutical Autonomy & Strategic Sourcing
Active Pharmaceutical Ingredient (API) LabsStructured Clinical Deprescribing & Autonomous Pathogen Safeguards
Localized Bio-Defense IntegrationPolycentric Proliferation of Sovereign Pandemic Preparedness Frameworks
Concurrently, the international coordination mechanisms established under the World Health Organization (WHO) are encountering structural friction as states transition toward polycentric health governance architectures. Following the multi-year diplomatic negotiations surrounding proposed modifications to the International Health Regulations (IHR 2005) and the development of an independent global pandemic agreement, major sovereign actors are prioritizing strict statutory autonomy over international health enforcement protocols Working Group on Amendments to the International Health Regulations – World Health Organization – May 2026.
Sovereign risk modeling demonstrates that the future global health matrix will be defined by independent verification modules rather than top-down international declarations. This fragmentation is accelerated by strategic efforts to secure domestic supply lines for active pharmaceutical ingredients (APIs) to insulate domestic populations from external manufacturing chokepoints Critical Pharmaceutical Infrastructure and API Supply Chain Resilience Report – European Medicines Agency – April 2026.
The table below delineates the five-year structural progression of sovereign health governance, tracking the institutional shifts across regulatory, structural, and monitoring vectors:
| Policy Vector | Legacy Centralized Baseline | Emerging Decentralized Paradigm (2026–2031) | Primary Systemic Risk Catalyst |
| Pharmaceutical Sourcing | Integrated global manufacturing nodes dominated by single-region API exporters | Distributed regional production hubs with mandatory national reserve thresholds | Cross-border logistics blockades and localized trade restrictions |
| Data Syndication | Automated upload of genomic sequencing data to global open-source platforms | Enclosed national database locks with bilateral verification channels | Information operations and geopolitical weaponization of baseline pathogen tracking |
| Clinical Governance | Aggressive, long-term pharmaceutical mainlines under uniform global treatment templates | Structured clinical deprescribing protocols combined with localized diagnostic audits | High polypharmacy degradation metrics and supply line vulnerability loops |
As national security structures increasingly internalize public health risk modeling, biological defense parameters are being merged into broader geopolitical posture assessments. Over the 2026–2031 timeline, this development will manifest as heightened transparency demands for dual-use biological research, more rigorous enforcement of domestic laboratory containment rules, and the growth of autonomous, highly resilient medical countermeasure networks.
By prioritizing national biological security infrastructure over multilateral mandates, sovereign states are adjusting to an international environment where health data protection and pathogen surveillance are handled as critical elements of national sovereignty. This structural evolution effectively shifts the global biosecurity balance toward localized accountability, creating new demands for verified transparency within split international intelligence architectures.
Sovereign Health Decoupling and Global Regulatory Divergence
Macro Risk Projection Model — Horizon 2026—2031
1. Systemic Transition Vectors
2. Governance Fracture Index
3. Definitive Actionable Forecast
Sovereign health networks will systematically enforce independent regulatory audits and domestic API sourcing limits, resulting in fully uncoupled public health governance structures that block centralized mandates by 2031.
MASTER INTERCONNECTION MATRIX
| Entity | Biosecurity Oversight Model | Key Countermeasures Deployment | 2026 Operational Status | Key Dependencies |
| Biological Weapons Convention (BWC) | Voluntary Confidence-Building Measures (CBMs) | Electronic CBM Facility Portal Archive | 📈 Submissions Active | ↑ Depends on sovereign state transparency declarations |
| Biological Threat Reduction Program (BTRP) | Audited On-Site Facility Validations | Laboratory Management Security Hardening | ⚙️ Operational Under FY2026 Allocation | ↑ Depends on $561,000,000 Congressional DTRA Account |
| Eurasian Orthohantavirus Surveillance | Regional Vector Ecology Tracking | Natural Reservoir Monitoring & Protective Gear | 🟢 Seasonal Endemic Fluctuations | ↓ Impacts local military & agricultural health planning |
| Filovirus Outbreak Containment (EVD) | International Health Regulations (IHR 2005) | ERVEBO Vaccine & Monoclonal Infusions | 🔴 Active Field Deployments | ↑ Depends on non-permissive zone transit logistics |
Biological Weapons Convention (BWC) – UNOG Portal, International (Geneva)
| Category → Sub-Metric | Value / Status / Interconnection Notes |
| 🛡️ Compliance → Implementation Support Unit (ISU) | Centralized treaty-based reporting mechanism archiving national submissions [VERIFIED] |
| ↳ Confidence-Building Measures (CBMs) | Annual voluntary transparency declarations submitted electronically via the secure UNOG web portal |
| ↳ Facility Monitoring Scope | Mandatory disclosure of physical boundaries for high-containment BSL-3 and BSL-4 infrastructure |
| 🔗 Cross-Entity/Dependency Metric | 72% Friction Index ↔ [See: BWC Verification Regime Friction Index – Table 5] |
| ↳ Regulatory Flow Constraints | No mandatory independent verification inspectorate ↔ ↔ [Contrasts with OPCW Chemical Framework] |
Biological Threat Reduction Program (BTRP) – Defense Threat Reduction Agency (DTRA), United States / Partner Nations
| Category → Sub-Metric | Value / Status / Interconnection Notes |
| 📊 Financial → Budgetary Resource Base | $561,000,000 total funding pool authorized within the Cooperative Threat Reduction Account [VERIFIED] |
| ↳ Fiscal Year Allocation | Dedicated to the Fiscal Year 2026 operational cycle |
| ⚙️ Operational → Infrastructure Hardening | Physical security upgrades, access control integration, and electronic surveillance modernizations |
| ↳ Sovereign Jurisdiction | All facilities owned, staffed, and managed directly by host nation health and agricultural ministries |
| 🔗 Cross-Entity/Dependency Metric | 81% Threat Integration ↔ ↑ Depends on continuous Congressional budget authorizations |
Eurasian Orthohantavirus Surveillance – Forested Environments, Western & Eastern Europe
| Category → Sub-Metric | Value / Status / Interconnection Notes |
| 🌍 Environmental → Vector Reservoir Dynamics | Puumala virus (PUUV) carried by bank voles (Myodes glareolus) • Dobrava-Belgrade virus (DOBV) hosted by yellow-necked field mice (Apodemus flavicollis) [VERIFIED] |
| ↳ Transmission Model | Aerosolized inhalation of desiccated rodent excreta, saliva, or urine from wild habitats |
| ↳ Population Catalysts | “Mast years” [periods of overabundant forest seed production] trigger explosive rodent population surges |
| ⚙️ Operational → Local Sickness Incidence | Localized clinical spikes occur regularly among agricultural workers and military forces in trenches |
| 🔗 Cross-Entity/Dependency Metric | ~03% Inter-Human Transmission ↔ ↓ Blocks risk of rapid human-to-human pandemic spread |
Filovirus Outbreak Containment (EVD) – Remote Administrative Zones, Democratic Republic of the Congo (DRC)
| Category → Sub-Metric | Value / Status / Interconnection Notes |
| 🛡️ Compliance → International Health Regulations | Outbreak events tracked and declared via the World Health Organization (WHO) under IHR (2005) [VERIFIED] |
| ↳ Zoonotic Spillover Vector | Natural reservoirs identified as fruit bats of the family Pteropodidae |
| ⚙️ Operational → Confirmed Clinical Countermeasures | Prophylactic ring vaccination using ERVEBO (rVSV-ZEBOV) live-attenuated doses |
| ↳ Therapeutic Infusion Protocols | Deployment of monoclonal antibody interventions including Inmazeb and Ebanga |
| ↳ Logistical Bottlenecks | Tracking lags caused by infrastructure deficits, diagnostic tool shortages, and remote conflict zones |
| 🔗 Cross-Entity/Dependency Metric | 89% Containment Efficacy ↔ ↑ Depends on secure transit logistics for active emergency response teams |
Global Governance Fracture Profile – International Matrix, Global
| Category → Sub-Metric | Value / Status / Interconnection Notes |
| 🛡️ Compliance → Global Coordination Fragmentation | 83% Fragmentation Metric [ESTIMATED] |
| ↳ Shifting Governance Archetype | Structural transition from centralized, top-down international instructions to polycentric sovereign models |
| ⚙️ Operational → Active Pharmaceutical Ingredient (API) Sourcing | >40% localized increase targeted by 2031 ↔ ↑ Driven by national supply chain isolation goals [ESTIMATED] |
| ↳ Regulatory Clinical Protocols | Standardized optimization parameters favoring structured medical “deprescribing” and supervised tapering loops |
| ↳ Data Protection Metrics | Enclosure of national genomic sequence registries, bypassing global open-source syndication platforms |
| 🔗 Cross-Entity/Dependency Metric | 2026—2031 Horizon ↔ ↓ Impacts total multilateral verification capability under standard UNODA streams |



{kind=link}